
BIOLOGICAL WARFARE AND ITS CUTANEOUS MANIFESTATIONS
Thomas W. McGovern, MD, MAJ, MC
George W. Christopher, LTC, USAF, MC
BIOLOGICAL WARFARE AND ITS CUTANEOUS MANIFESTATIONS
Thomas W. McGovern, MD, MAJ, MC
George W. Christopher, LTC, USAF, MC
Key Words: biological warfare, cutaneous manifestations, hemorrhagic fever, mycotoxins, poxviruses, plague, melioidosis
INTRODUCTION
Biological warfare agents have gained attention in recent years. They have been discussed in Congress and in the medical literature, and have been the subject of frequent commentaries.[109] The mention of ‘biological warfare’ often elicits a sense of deadly mystery, as summarized by a Russian journalist
"I have been gathering information on bacteriological weapons (BW) for several years. Out of all the means of mass destruction, this kind can be considered as the most mysterious."[112]
This article attempts to eliminate some of that mystery by discussing the history and background of biological weapons and by reviewing agents that cause cutaneous disease. While a biological attack could result in a made-made epidemic of unprecedented scale, the classical principles of clinical medicine and epidemiology would apply. Prompt diagnosis and early interventions could reduce morbidity and mortality, and mitigate the effects of a biological attack. In the aftermath of a biological attack, dermatologists could play a critical role in recognizing the differential diagnosis of an epidemic exanthem and alerting public health officials, leading to prompt medical and public health interventions, hopefully preventing wide-spread mortality.
History
‘Biological Warfare’ (BW) is defined as the ’employment of biological agents to produce casualties in man or animals or damage to plants.’[91] An early BW attack took place in the Black Sea port of Kaffa (now Feodossia, Ukraine) in 1346. Rats and their fleas carried the disease to attacking Tatar soldiers. In spite, the Tatars catapulted the bodies of victims at the defending Genoese who contracted plague and left Kaffa. The same rats afflicting the Tatars likely brought disease to the Genoese.[5]
Another attempted use of biological warfare occurred between 1754 and 1767 when the British infiltrated smallpox-infested blankets to unsuspecting American Indians during the French and Indian war. Smallpox decimated the Indians, but it is unclear if the contaminated blankets or endemic disease brought by the Europeans caused these epidemics.[92] In 1932, the Japanese began a series of horrific experiments on human beings at ‘Unit 731’ outside Harbin, Manchuria, China.[92] At least 11 Chinese cities were attacked with the agents of anthrax, cholera, shigellosis, salmonella, and plague, and at least 10,000 died during their gruesome experiments.[27]
The United States started an offensive biological warfare program at Camp Detrick (today Fort Detrick) in Frederick, Maryland in 1943.[27] Ten years later, the defensive program began. By 1969, the U.S. had weaponized the agents causing anthrax, botulism, tularemia, brucellosis, Venezuelan equine encephalitis, and Q fever.[92]
|
|
 2b
2b |
Figures 2a, 2b: The "eight ball" one million liter test sphere at Fort Detrick, Maryland. Animals were tethered within the sphere while aerosolized agents were aerosolized. |
 |
Figure 3: Anthrax pilot plant used to produce billions of anthrax spores at Fort Detrick, Maryland before the United States unilaterally ended offensive BW research in 1969. Spores were sent to other military sites where they were placed in weapons. The building is entirely free of anthrax spores and on the National Register of Historical Places. Tours frequently take visitors through this old production facility. |
These were soon destroyed after President Nixon unilaterally ended the U.S. offensive biological warfare program that year.[74] 1972 the U.S. signed the Biological Weapons Convention stating that it would never develop, produce, stockpile, acquire, or retain BW agents or the means to deliver them.[74]
Despite this convention, the development of BW weapons has continued. Controversial evidence suggests that ‘yellow rain’ (trichothecene mycotoxins) attacks in Southeast Asia caused thousands of deaths between 1974 and 1981.[8] In 1978, Bulgarian dissident Georgi Markov was assassinated using an ‘umbrella gun’ that shot ricin into his thigh.[92] At least 66 people died of inhalational anthrax when an aerosol of Bacillus anthracis spores was accidentally released from a BW research facility in Sverdlovsk, USSR in 1979.[92]
By 1991, the Iraqis had weaponized anthrax, botulinum toxin, and aflatoxin.[110] Fortunately, these were not used during Desert Shield or Desert Storm. The United Nations destroyed the final remains of the Iraqi offensive program in 1996.
 |
Figure 1: Al Hakam Single-Cell Protein Plant. Iraq's major facility for the production of biological warfare agents. Under the watchful eye of the United Nations Special Commission, this plant was destroyed by Iraqui workers in May and June of 1996. (Photo courtesy of Davis Franz, DMV, PhD) |
Finally, in 1995, the Aum Shinrikyo cult, that released sarin nerve gas in a Japanese subway, was found to possess rudimentary biological weapons including anthrax, botulism, and Q fever.[92]
Advantages of Biological Warfare[91,105,106,109]
BW agents can cause large numbers of casualties with minimal logistical requirements. Perpetrators can escape long before BW agents cause casualties, due to the incubation periods of the agents. Weapons are easy and cheap to produce and can be used to selectively target humans, animals, or plants. The costs of conventional weapons ($2000), nuclear armaments ($800), and chemical agents ($600) would far outstrip the bargain-basement price of biological weapons ($1) to produce 50% casualties per square kilometer (1969 dollars).[91]
Agents can be easily procured from the environment, universities, biological supply houses, and clinical specimens.[105] In fact, a white supremacist (who happened to be a microbiologist) received a vial of Yersinia pestis shipped to his home by the American Type Culture Collection in Rockville, MD.[113] Common fermentation techniques used for producing antibiotics, toxoid vaccines, foods, and beverages can be used to grow large quantities of biological agents. Simple aerosol generating devices mounted on planes or trucks, as used for crop-dusting, can generate 1-5 micron particles ideal for causing infectious aerosols.[111] Aerosol particles 0.5-5 microns in diameter settle in the alveoli; larger particles are cleared by respiratory mucosa, and smaller particles float in and out of the alveoli without settling. BW agents are typically invisible in aerosol clouds and may not be detected until humans become ill. Panic would result as medical capabilities are quickly overwhelmed.
Disadvantages to using BW agents as weapons include hazards to the user, their dependence on optimal weather conditions to result in effective dispersal, and their possible inactivation by solar irradiation and other climatic conditions. BW attacks would most likely occur late at night or early in the morning when agents would be less likely to undergo inactivation by ultraviolet radiation. At these times, atmospheric temperature inversions would allow an agent cloud to travel at low altitude to cover its target.
Selecting a BW Agent[9,105,106,111]
Pathogens may be used against personnel, animals, or plants. Agents may kill or incapacitate victims. Incapacitating agents may be more effective in battle by both preventing a unit from carrying out its mission and overwhelming medical and evacuation assets. Agents with short incubation times would be most effective in a tactical setting, while those with longer incubation periods would appeal more to terrorists.[111]
Biological attacks against large populations would most likely be disseminated by aerosol. A respiratory portal of entry may cause different clinical features than naturally occurring disease (e.g. anthrax occurs mainly as a cutaneous disease in nature, but causes a rapidly lethal hemorrhagic mediastinitis when spores are inhaled).
Biological attacks could be attempted by contaminating food and water supplies, although modern water purification and the dilution effects in large volumes of water would negate the effectiveness of a water-borne attack.[109] While intact skin is an excellent barrier to most biological warfare agents, some agents, such as trichothecene mycotoxins, can penetrate the integument and cause systemic illness. Ingestion and cutaneous penetration are currently considered unimportant potential routes of exposure.[105] More unusual methods of dispersion could include releasing agents in their natural arthropod vectors.
Person-to-person transmission of several agents ( notably plague and smallpox) could perpetuate an epidemic. Nosocomial transmission could result from blood and body fluid exposures (hemorrhagic fever viruses, smallpox, and plague).
In 1970, WHO predicted that a city of 500,000 people would be devastated following an aerosol release of as little as 50 kg of BW agent (Table 1).[107]
Is There a Real Biological Warfare Threat?
Current unclassified information reveals that, despite the 1972 Geneva Biological Weapons Convention, at least seventeen countries are known or suspected of having offensive biological weapons programs.[104] Clearly, BW is a credible threat to our military, as it was during Desert Shield/Storm.[110] Terrorist use of BW agents could kill many people to create an unparalleled medical, political, and social crisis. Despite the fact the biological weapons have never been used against the United States,[111] we must prepare for a new age of terrorism.[105,106,109] Civilian health-care workers must know how to recognize a BW attack in the event of terrorist use of BW agents on civilian populations.[109]
Current U.S. Biological Warfare Policy
The U.S. government currently states that nuclear warfare would be used only as a ‘last resort’, and chemical warfare might be used to retaliate an enemy’s first use of chemical agents. However, the U.S. has vowed to never use BW agents under any circumstances. All BW agent work is limited to defensive measures such as developing immunizations, detection methods, personal protective equipment, decontamination, rapid diagnostic tests, and treatments.[74]
United States Defensive Program
 |
Figure 4: Entrance to Fort Detrick with headquarters building in background. |
The U.S. BW defense program is centered at Fort Detrick, MD at the United States Army Medical Research Institute of Infectious Diseases (USAMRIID). No classified work is done; all research is open; investigators are encouraged to present their findings at scientific meetings and in peer-reviewed journals.[74] Information is regularly shared with foreign visitors and collaborators. Its mission is to conduct research to develop strategies, products, information, procedures, and training for medical defense against biological warfare agents (90%) and naturally occurring agents of military importance that require maximal containment for laboratory safety (10%).[91,105]
 |
Figure 5: Front of main building at USAMRIID (United States Army Medical Research Institute of Infectious Diseases) on the grounds of Fort Detrick, Maryland. |
USAMRIID offers a biological warfare defense course that reviews agents most likely to be used by an enemy military. The agents listed in Table 2 have detailed clinical data sheets in the NATO handbook on biological warfare defense[91], are included in the Textbook of Military Medicine Volume entitled ‘Medical Aspects of Chemical and Biological Warfare,[111] and/or are taught at the US Army’s Management of Chemical and Biological Casualties Course.
AGENTS WITH CUTANEOUS MANIFESTATIONS AS PART OF A BW PRESENTATION
BACTERIAL AGENT – Burkholderia pseudomallei
Burkholderia (formerly Pseudomonas) pseudomallei is a gram-negative bacillus isolated from soil, stagnant streams, ponds, rice paddies, and market produce in endemic areas and can cause epizootics in sheep, goats, swine, horses, and seals.[4,33,43,45,77] Humans contract disease from contamination of abrasions with soil but may also ingest or inhale organisms.[4,45] Melioidosis is endemic to southeast Asia and northern Australia, but it may occur anywhere between 20 degrees north and south latitudes.[4,45] It is most widespread in Thailand where it accounts for 19% of hospitalizations and 40% of deaths from community-acquired septicemia.[4] Mild or subclinical infections are common; 80% of Thai children are seropositive by age five years.[4]
Melioidosis most commonly presents as an acute pulmonary infection, but it may present as an acute localized skin infection or septicemia. Chronic suppurative infections often develop with secondary abscesses in the skin, brain, lungs, myocardium, liver, spleen, bones, lymph nodes, or eyes.[4] Melioidosis may remain latent for years. Even months of treatment with appropriate antibiotics do not necessarily eradicate the disease. Histologically, caseating granulomas as found in tuberculosis are seen. Melioidosis has been called the ‘Great Imitator’ because the disease does not show any specific clinical features except perhaps the presentation of suppurative parotitis in children.[43] Fulminant respiratory failure, multiple pustular and necrotic skin lesions, or the radiologic appearance of tuberculosis without isolating any mycobacteria suggests the diagnosis of melioidosis.[4,43,45] Definitive diagnosis requires culturing organisms from blood or body fluids. No carrier state exists; recovery of organisms denotes active disease.[77]
Antibiotic treatment should be based on sensitivities. Ceftazidime has been most responsible for reducing mortality. Treatment must continue at least 30 days, but 60-150 days is recommended for pulmonary disease and 6-12 months for suppurative extrapulmonary disease.[45] Before antibiotics, 95% of patients died. The mortality rate for septicemic disease is over 50% and 20% for localized disease despite treatment. Overall, mortality is 40%. There are no available vaccines.[43,45,77]
Cutaneous Manifestations
Severe urticaria has been reported with pulmonary melioidosis.[93] Flushing and cyanosis may develop during septicemia. No cutaneous lesion, however, is specific or diagnostic of melioidosis, nor is any likely to be present with acute pulmonary disease. Inhalational melioidosis could lead to any of the skin manifestations mentioned below, but only after metatstatic abscesses to the skin formed, and this would likely take months. Many patients in endemic areas present with pustules or cutaneous abscesses associated with lymphangitis, cellulitis, or regional lymphadenitis.[77] Draining sinuses from lymph nodes or even bone may be present. Abscesses may ulcerate, and rarely, ecthyma gangrenosum-like lesions may form.
BW considerations
B. pseudomallei would most likely be delivered as an aerosol. However, its long incubation period would make it a less effective agent than anthrax. The lack of a vaccine and its high mortality despite treatment may increase its utility as a BW agent. Acute pneumonia could be confused with plague given the similar appearance of stained organisms.
BACTERIAL AGENT – Yersinia pestis
Because of its high mortality (approximately 200 million deaths throughout history)[57], Yersinia pestis has attracted attention for development as a possible BW agent.
This gram-negative bacillus develops an anti-phagocytic carbohydrate protein envelope (F1 capsular antigen) during growth above 33o C.[57] A single gene encodes the Pla protease that provides both fibrinolytic and coagulase activities. At 37o C, fibrinolysis is most active; at 28o C, coagulation predominates. This enzyme helps organisms grow and remain in flea guts or spread through tissues in mammals. Other virulence factors act in concert with these such that only 2-10% of the bacteria needed to cause death in mammals at 25o C is necessary at 37o C.[57]
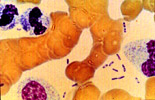 |
Figure 6: Wright's stain peripheral blood smear of a patient with septicemic plague demonstrating bipolar, safety-pin staining of Yersinia pestis. While Wright's stain will often demonstrate this characteristic appearance, Giemsa's and Wayson's stains most consistently highlight this pattern. (Courtesy Ken Gage, PhD., CDC, Fort Collins, CO. ) |
At least 30 types of fleas and over 200 species of mammals in 73 genera serve as reservoirs.[60] Flea infection is restricted to the alimentary canal where bacilli either are passed or stay in the midgut (stomach). There they multiply in a fibrinoid mass of blood on needle-like spines in the proventriculus. These spines aid the rupture of red blood cells and normally prevent the regurgitation of a blood meal. Such ‘blocked’ fleas cannot digest their food and ultimately die. However, this state makes them ravenously hungry. In an attempt to feed, blood sucked from a mammalian host mixes with bacilli which are regurgitated back into the host. Fleas become unblocked and plague transmission ceases at temperatures above 28o C.[137] This may be caused by differential effects of Pla protease at different temperatures.[5,57]
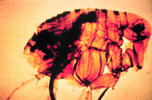 |
Figure 7: Here a flea is shown with a blocked proventriculus, equivalent to the gastroesophageal region in man. In nature, this flea would develop a ravenous hunger because of its inability to digest the fibrinoid mass of blood and bacteria. Ensuing biting of the nearest mammal will result in clearing of the proventriculus through regurgitation of thousands of bacteria into the bite wound. (Courtesy United States Army Environmental Hygiene Agency) |
After a flea injects a blood meal into an unsuspecting host, neutrophils and monocytes engulf the bacilli and transport them to regional lymph nodes. While the neutrophils can destroy bacilli, the monocytes cannot. In monocytes, Y. pestis multiplies and develops its anti-phagocytic capsule that prevents even neutrophils from digesting it. Bacilli then multiply in lymph nodes and the blood and travel throughout the body, but especially to the spleen, liver, lungs, and meninges.[5,57]
Every continent except Australia and Antarctica maintains enzootic foci of plague.[57] Between 1979 and 1993, 16,312 worldwide cases resulted in over 1600 deaths.[57]
Clinical Features
Most endemic plague presents with tender, erythematous lymphadenopathy, most commonly in the groin and causes bubonic plague (Greek boubon = groin). Buboes may point and drain spontaneously. [103] Bubo location is primarily a function of the region of the body in which an infected flea inoculates plague bacilli.
 |
Figure 8a: Bubo of femoral lymph nodes, the most common site of erythematous, tender, swollen nodes in a plague victim. |
 |
8b: The next most common lymph node regions involved are the inguinal, axillary (b) and cervical areas. This child has an erythematous, eroded, crusting, necrotic ulcer at the presumed primary inoculation site on the left upper quadrant. This type of lesion is uncommonly found in patients with plague. (Photos courtesy of Ken Gage, PhD., CDC, Fort Collins, CO) |
 |
Figure 9: Small femoral bubo and presumed inoculation site (inferior thigh) in a patient with plague pneumonia. No chest x-ray pattern is characteristic of plague, but bilateral interstitial infiltrates are most commonly seen. (Photos courtesy of Ken Gage, PhD., CDC, Fort Collins, CO) |
A lesion is seen at the site of a flea bite no more than 10% of the time.[102] Spread to the bloodstream results in septicemic plague.[104] From the blood, the meninges may become infected. Spread to the lungs results in pneumonic plague that is rapidly fatal and transmissible. Because bacilli in pneumonic plague lesions possess an anti-phagocytic capsule, transmission by cough or sneeze can lead to death in a healthy individual within one to two days. The median infective inhaled dose is 100-500 bacilli.[105] However, as only 1-10 bacilli can infect rodents or primates via the oral, intradermal, subcutaneous, or intravenous route.[138] Respiratory droplets can be inhaled by those within two to five feet. The ensuing flu-like illness progresses rapidly to overwhelming pneumonia with cough and bloody sputum. If not treated within 24 hours of symptoms, pneumonic plague patients almost all die.[105,137] One must have a high index of suspicion to diagnose plague in the absence of buboes. Stains and cultures of blood, bubo aspirates, sputum, cerebrospinal fluid, or even skin scrapings may be helpful in isolating the organism.
The formalin-killed plague vaccine protects against bubonic, but not inhalational plague.[139,140,141] Attempts at more immunogenic live-attenuated vaccines result in no increase in immunogenicity and sporadic reversion of vaccine strains to virulent, wild type bacteria.[142] Most strains of Y. pestis are sensitive to streptomycin, gentamicin, tetracycline, chloramphenicol, trimethoprim/sulfamethoxazole, and doxycycline. Although in vitro testing has demonstrated the effectiveness of quinolones, rifampin, third-generation cephalosporins, and amoxicillin, these have not been used to any great degree in human cases.[5] The U.S. military currently requires the vaccine only for those traveling or deploying to high risk areas and for those employed in high risk occupations (entomologists or laboratory workers using Y. pestis).[20]
Cutaneous Manifestations
Terminal pneumonic and septicemic plague patients, as would be seen in a BW scenario, would develop livid cyanosis and large ecchymoses on the back.[96] Septicemia could cause petechiae, purpura, ecchymoses, and acral necrosis. [103,137]
 |
Figure 10: Ecchymoses at the neck base of a girl with plague. Bandage is over the site of a prior bubo aspirate. These lesions probably gave rise to the title line of the children's nursery rhyme "ring around the rosy". (Photos courtesy of Ken Gage, PhD., CDC, Fort Collins, CO) |
No chest x-ray pattern is characteristic of plague, but bilateral interstitial infiltrates are most commonly seen.
 |
Figure 11: Right-side, middle and lower lobe involvement in a patient with plague pneumonia. (Photo courtesy of Ken Gage, PhD., CDC, Fort Collins, CO) |
 |
Figure 12: Rock squirrel in extremis coughing up blood-streaked sputum of pneumonic plague. (Photo courtesy of Ken Gage, PhD., CDC, Fort Collins, CO) |
Rare cases of ecthyma gangrenosum-like lesions and carbuncles due to plague have been reported.[96,103]
 |
|
| Figures 13a, b: Acral necrosis of the nose, lips, fingers (a) and toes (b) and residual ecchymoses over both forearms in a patient recovering from bubonic plague that disseminated to blood and lungs. At one time, the patient's entire body was ecchymotic. (Reprinted from McGovern TW, Friedlander AM. Plague. In: Sidell FR, Takafuji ET, Franz DR, eds. Medical Aspects of Chemical and Biological Warfare. Chapter 23 In: Zajtchuk R, Bellamy RF, eds. Textbook of Military Medicine. Washington, DC: US Department of the Army, Office of the Surgeon General, and Borden Institute; 1997:493. | |
Pharyngitis associated with cervical lymphadenopathy has been reported in contacts of bubonic plague patients.[143] Of course the most common cutaneous manifestation of plague, the bubo, would not be present in a BW scenario unless the Japanese plan (discussed below) of releasing infected fleas was resurrected.
BW considerations
While Yersinia pestis would most likely be aerosolized for a BW attack, the Japanese employed a more creative approach in China during World War II. Human fleas (Pulex irritans) were multiplied and then infected with Y. pestis. These organisms were released into several Chinese cities where small epidemics of plague ensued. Normally, animal hosts die in epizootics before humans are infected, but in these cases, humans died first and then animals began dying of plague.[5,97]
Plague would most likely be transmitted as an aerosol in the event of BW.[105] The possibility of rapid death combined with possible person-to-person transmission (in contrast to anthrax) make plague an ominous BW threat. The United States studied Y. pestis as a potential offensive weapon in the 1950s. Other countries are suspected of weaponizing plague.[105]
TOXIN THREAT – Trichothecene mycotoxins
Trichothecene mycotoxins (‘Yellow Rain’) are the only potential BW toxins with cutaneous activity and manifestations. Mycotoxins are a diverse group of small molecular weight compounds produced by fungi.[52] They can occur at toxic levels in moldy grains and other agricultural products[8,52] and are mainly produced by members of five fungal genera: Aspergillus, Penicillium, Fusarium, Alternaria, and Claviceps.[52] Eating contaminated foodstuffs and perhaps inhaling aerosolized toxins uncommonly causes natural human or animal disease.[7,8,52]
Clinical Features
Human intoxication is rare. An entity known as alimentary toxic aleukia, reported in Russia since the 19th century, is thought to result from ingestion of mycotoxins while eating foods prepared from moldy grain. Signs and symptoms include vomiting, diarrhea, ‘skin inflammation,’ leukopenia, hemorrhage, and sepsis.[8,52]
More recently, and closer to home, trichothecene mycotoxins are thought to have caused fatal pulmonary hemorrhage in Cleveland area infants. In one area of Cleveland, it may have accounted for 5% of cases of sudden infant death syndrome between 1993-95. In all cases, the fungus Stachybotrys atra was found growing in water-saturated cellulose in the walls of poorly maintained homes.[7,29,31]
Cutaneous Manifestations
At low doses (nanograms), severe skin irritation with erythema, edema, and necrosis is observed. Vesication often occurred with ‘Yellow Rain’ attacks; T-2 (one of the trichothecenes) mycotoxin is estimated to be 400 times more potent than alkylating agents (mustards) in producing skin injury.[99]
 |
Figure 14: Vesicles and erosions on the back of hairless guinea pigs at 1,2,7 and 14 days after application of ( bottom to top) 25, 50, 100 or 200 ng of T-2 mycotoxin in 2ul of methanol. (Reprinted from McGovern TW, Friedlander AM. Plague. In: Sidell FR, Takafuji ET, Franz DR, eds. Medical Aspects of Chemical and Biological Warfare. Chapter 23 In: Zajtchuk R, Bellamy RF, eds. Textbook of Military Medicine. Washington, DC: US Department of the Army, Office of the Surgeon General, and Borden Institute; 1997:493. |
BW considerations
Epidemiologic, intelligence, and trichothecene assay evidence suggest that trichothecene mycotoxins were used in Southeast Asia between 1974 and 1981.[8,91] Nearly 400 alleged attacks reportedly resulted in approximately 10,000 deaths. In Laos, the attacks were described as ‘yellow rain,’ a sticky yellow liquid that fell and sounded like rain or looked like a yellow cloud of dust, powder, mist, smoke, or insect spray. The liquid dried rapidly to form a powder. Most attacks used yellow pigment, but some attacks used red, green, white, or brown smoke or vapor. More than 80% of attacks were by air to surface rockets.[98]
Microgram exposure caused eye irritation, corneal damage, and impaired vision. At 0.1-0.2 LD50, emesis and diarrhea occurred. Aerosols caused death within minutes to hours by destroying alveoli. The toxins affect rapidly proliferating tissues and are cytotoxic to most eukaryotic cells by inhibiting protein and RNA synthesis. After entering the circulation, regardless of portal of entry, they affect all rapidly proliferating tissues.
A protective mask and full-body clothing should be donned at the first sign of a ‘yellow rain’ attack. Afterwards, battle dress uniforms (BDUs) and contaminated areas of skin should be washed with soap and water followed by a water rinse. Washing within 4-6 hours of exposure removes 80-98% of the toxin and prevented death and dermal lesions in experimental animals. No known specific therapy exists, although high doses of systemic steroids decreases primary and secondary toxin injury.[8]
VIRAL AGENTS – Poxviridae
Poxviruses, the largest of all viruses, differ from other DNA viruses by replicating in the cytoplasm where they produce eosinophilic inclusion bodies. They are relatively resistant to drying and many disinfectants.[14] The Orthopox genus includes at least nine species.[118] Three viruses interest us in a BW context: variola, monkeypox, and vaccinia.
Variola is an orthopox virus very similar to vaccinia but with different host predilections.[16] There was no animal reservoir (although monkeys are susceptible to infection); this factor enabled global eradication of this disease. Variola retains its transmissibility for one year in dust and cloth.[10] Person-to-person transmission requires close contact.[16] Patients were most infective 4-6 days after the illness started, and respiratory spread was probably the most common route of transmission. Only 30% of susceptible contacts became infected.[18]
Monkeypox was first identified in 1958 as a pathogen of cynomolgus monkeys; in 1971 it was linked to human disease.[17] The virus exists in an enzootic state in arboreal squirrels of tropical rain forests of western and central Africa.[2,17] Person-to-person transmission by respiratory droplet occurs.[16,17]
Clinical Features/Cutaneous Manifestations
Thirty years ago, smallpox was endemic in 31 countries affecting 15 million people each year (of which 2 million died). Survivors often remained disfigured or blinded for life. A 10-year WHO program eradicated the disease as of October, 1977.[11,18]
Smallpox featured an incubation period of 7-17 days and a prodrome of 2-4 days. During the prodrome, 10% of light-skinned patients develop an erythematous rash.[121] An enanthem on the buccal and pharyngeal mucosa started on about the second day. These lesions shed virus and allowed for aerosol spread, the most important means of viral transmission.[122] The typical lesions started on the face, spread to the forearms and hands, and finally appeared on the lower limbs and trunk within about one week. Macules progressed to papules, vesicles, pustules (sometimes umbilicated), and crusts distributed in a centrifugal pattern (in distinction to varicella) over a 1-2 week period.
 |
Figure 15: Electron micrograph of pox virus |
Several clinical varieties of smallpox were described. ‘Ordinary’ smallpox (variola major), present in 80% of patients, led to 3% mortality among the vaccinated but 30% among the unvaccinated.
|
16a. |
16b. |
16c. |
Figures 16a-c: Unvaccinated infant with centrigugally-distributed umbilicated pustules on days 3 (a), 5 (b) and 7 (c) of 'ordinary' form of variola major strain of smallpox. (Reprinted with permission from Fenner F, Henderson DA, Arita I, Jezek Z, Ladnyi ID. Smallpox and its eradication. Geneva, Switzerland: World Health Organization; 1988:10-14. Photographs by I. Artia) |
 |
Figure 18: Adult with variola major lesions. Death usually ensued before typical pustules developed. (Reprinted with permission from Fenner F, Henderson DA, Arita I, Jezek Z, Ladnyi ID. Smallpox and its eradication. Geneva, Switzerland: World Health Organization; 1988:10-14. Photographs by I. Artia) |
The most virulent form, hemorrhagic smallpox, was seen in less than 3% of patients. 96% of these patients died, usually before they developed typical pox lesions.[124]
 |
Figure 19:Hemorrhagic-type variola major lesions. Death usually ensued before typical pustules developed. (Reprinted with permission from Fenner F, Henderson DA, Arita I, Jezek Z, Ladnyi ID. Smallpox and its eradication. Geneva, Switzerland: World Health Organization; 1988:10-14. Photographs by I. Artia) |
Flat smallpox occurred in 2-5% of patients with severe systemic toxicity and slow evolution of flat, soft, focal skin lesions.[114] 66% of the vaccinated and 95% of the unvaccinated died. Alastrim, or variola minor, was a mild illness featuring diminutive cutaneous lesions, mild systemic disease, and a case fatality rate of less than 5%.
|
|
|
Figures 17a,b: 'Ordinary form' of variola minor strain of smallpox (alastrin) in an unvaccinated woman 12 days after the onset of skin lesions. The facial lesions are more sparse (a) and evolved more rapidly than the extremity lesions (b). (Reprinted with permission from Fenner F, Henderson DA, Arita I, Jezek Z, Ladnyi ID. Smallpox and its eradication. Geneva, Switzerland: World Health Organization; 1988:10-14. Photographs by I. Artia) |
Monkeypox greatly resembles variola with a pustular eruption, fever, respiratory symptoms, and death in 3-10% of cases.[118]
|
|
 20b 20b |
Figure 20a,b: Boy with monkeypox in Democratic republic of the Congo in 1996. Note the centrifugal distribution and synchronicity of lesions as was typical for smallpox. (Courtesy of William Clemm). |
The only distinguishing feature appears to be cervical and inguinal lymphadenopathy.[105,118] Secondary bacterial pneumonia is associated with a 50% mortality. An outbreak in Zaire between February and August 1996 led to 71 cases with 6 deaths in 13 villages in a region of 15,000 people.[17] Unlike smallpox, monkeypox possesses a non-human reservoir, an arboreal squirrel.[119] In February, 1997, a search in 12 villages found 92 possible cases among 4000 people (2% attack rate). Fifteen of 84 had a smallpox vaccination scar.[17] Communicability may be related to declining vaccinia-induced immunity.[2,105] Vaccinia immunization seems to provide 85% protection against monkeypox.[120]
BW considerations
Smallpox has been eradicated, but at least two sites, the Centers for Disease Control and Prevention in Atlanta and the Russian State Research Center of Virology and Biotechnology in Koltsovo, Russia still maintain viable variola. The extent of clandestine stockpiles remains a matter of debate and concern.[105] WHO has set June 30, 1999 as the day all variola stocks are to be destroyed.[11] If variola were ever released by an enemy or by terrorists, morbidity and mortality could be considerable. The person-to-person aerosol infectivity, high mortality, and stability make variola (and possibly monkeypox) a potential BW threat.[118] Other animal poxviruses could be genetically engineered to be virulent in humans.[105] While WHO has 200-300 million doses of smallpox vaccine stored, the vaccine is gradually losing virulence, and the number of smallpox-naïve individuals continues to increase as vaccination has virtually ceased.[117]
VIRAL AGENTS – Hemorrhagic fever viruses
Hemorrhagic fever (HF) is a clinical syndrome featuring fever, myalgia, malaise, hemorrhage, and in some cases, hypotension, shock and death. The hemorrhagic fever viruses belong to four families of lipid enveloped viruses with single-stranded RNA genomes.[129] The taxonomy, ecology, and epidemiology of these viruses are summarized in Table 3. Transmission of HF viruses varies with the specific virus. However, all of the HF viruses, with the exception of dengue, are potentially transmitted via aerosol, underscoring their possible role as BW agents.[129]
Hemorrhagic fever viruses are transmitted by arthropod vectors or contact with infected animal reservoirs.[105] Arenaviruses and Hantaviruses are transmitted by inhalation of aerosolized rodent excreta, while Rift Valley Fever and Congo-Crimean hemorrhagic fever (CCHF) can be aerosolized during the butchering of infected livestock.[129] The reservoir for filoviruses remains a mystery.[10,30,44,56,59,84] Person-to-person spread may occur via direct contact with infected patients or their blood and body fluids.[25,32] Four viral hemorrhagic fevers (VHFs) have a high risk of nosocomial spread and are quarantinable conditions: Lassa fever, CCHF, Ebola fever, and Marburg disease.[44,59] While epidemiologic studies indicate that respiratory transmission of viral hemorrhagic fevers does not occur among humans, such transmission has occurred among non-human primates. In addition, subclinical human infections due to a filovirus virulent for monkeys (Ebola-Reston) have occurred after respiratory exposure to infected animals.[130]
|
|
|
|
Figure 21: Site of Lassa Fever outbreak in Liberia, 1988. (Courtesy Peter B.Jahrling, PhD.) |
Figure 23: The fertile Pampas of Argentina, site of the Argentine Hemorrhagic Fever due to Junin virus. (Courtesy Peter B.Jahrling, PhD.) |
The potential risk of person-to-person transmission of zoonotic viruses is underscored by a recent report from Argentina suggesting secondary transmission of hantavirus pulmonary syndrome, resulting in 15 cases and 8 deaths. In addition, infectious aerosols may be generated during endotracheal suctioning and other medical procedures. Although nosocomial transmission of HF in Africa has been interrupted by standard universal precautions without additional respiratory measures, adding respiratory protection as an infection control measure is advised by the Centers for Disease control and Prevention because information regarding exposure and transmission in humans is limited. Infections can be prevented by avoiding contact with vectors and reservoirs, practicing standard hospital infection control procedures, patient isolation, disinfection, and reporting cases to public health officials.[25,44]
Clinical Findings
Viral hemorrhagic fevers present as acute febrile illnesses characterized by malaise, myalgias, and prostration dominated by generalized abnormalities of vascular permeability because the target organ for viral replication is the endothelial cell.[105,129,136] Initial signs include flushing, conjunctival injection, periorbital edema, petechiae, hypotension, and a positive tourniquet test. Early in the disease course, signs and symptoms are non-specific and make differentiation from endemic febrile illnesses (malaria, enteric fever, typhoid fever, meningococcemia, rickettsioses, other viral infections, and non-infectious diseases such as vasculitis, thrombotic thrombocytopenic purpura, hemolytic uremic syndrome, and heat stroke) very difficult.[59,129] Full-blown disease develops into shock and generalized mucosal hemorrhage. Neurologic, hematopoietic, or pulmonary involvement is often present. Diffuse bleeding often occurs as a result of widespread vascular damage, hepatic dysfunction and/or disseminated intravascular coagulation (DIC). Life-threatening blood loss rarely occurs.[105]
Some clinical features may differentiate the hemorrhagic fevers. An exanthem is common with the filoviruses,[56,84,89,90] sometimes occurs in hemorrhagic fever with renal syndrome and dengue fever,[44] is uncommon with Lassa fever,[59] and is absent in CCHF. Capillary leak syndrome is most common in Lassa fever while hemorrhage and neurological manifestations are uncommon.[59,105] Neurologic and hemorrhagic complications are common among the South American Arenaviruses.[105] Rift Valley Fever rarely causes hemorrhage.[129] While CCHF exhibits no edema, it results in DIC and the most severe hemorrhage among HF viruses.[59] Filoviruses also exhibit significant DIC.[56,89,90,129]
Sequelae of VHFs include hair loss, Beau’s lines, deafness (Lassa, Ebola), retinitis (RVF, KFD), uveitis (RVF, Marburg), encephalitis (AHF, BHF, RVF, KFD, and OHF), pericarditis (Lassa), and renal insufficiency (HFRS).[129]
Treatment is supportive with special attention to fluid and electrolyte balance, and treatment for shock, blood loss, renal failure, seizures, and coma. These may require intensive care interventions such as mechanical ventilation, dialysis, and neurological support.
The role of heparin therapy for DIC is controversial and should be reserved for patients with clinically significant hemorrhage and laboratory evidence of DIC. Aspirin and other medications that impair platelet function are contraindicated, as are intramuscular injections. The use of intravascular devices needs to be carefully considered in the context of potential benefit versus the risk of hemorrhage. Surgical interventions should be offered if indicated.[25,129]
Specific antiviral therapy is limited. Clinical studies support the use of intravenous ribavirin for the treatment of Lassa fever, Argentine and Bolivian hemorrhagic fevers, hemorrhagic fever with renal syndrome due to Hantaan virus, and CCHF.[131] Intravenous and oral ribavirin are available through human use protocol only but are reasonable options for any infection due to an Arenavirus or Bunyavirus.[129]
Immunotherapy with convalescent plasma has been beneficial in the treatment of Argentine and Bolivian hemorrhagic fevers.[129,133] Passive immunization does not work, however, for Lassa fever[134] or CCHF.[135]
A live attenuated yellow fever vaccine is the only licensed immunization for the viral hemorrhagic fevers available in the United States. A live, attenuated vaccine against Argentine Hemorrhagic Fever (Junin virus) has proven safe and effective in endemic areas. It also protects monkeys against aerosol exposure to Bolivian Hemorrhagic Fever (Machupo).[129] Other investigational vaccines include a formalin-inactivated vaccine and a live attenuated vaccine for Rift Valley fever and a vaccinia-vectored vaccine against HFRS due to Hantaan virus.[44,129]
Cutaneous Manifestations
Hemorrhagic fevers may produce a variety of cutaneous manifestations. Most of these are due to vascular instability and bleeding. Flushing, petechiae, purpura, ecchymoses, and edema may occur in the discussed diseases except for Rift Valley Fever. No skin manifestations are typically associated with this disease.[44]
Lassa Fever patients have a high incidence of facial edema, probably due to extensive capillary leak
Figure 22: Old World Arenavirus-Lassa Fever. Patient
with Lassa Fever during an outbreak in Liberia in 1988. Note the periorbital
edema and conjunctival hemorrhage. Lassa fever patients typically exhibit
significant edema without hemorrhagic manifestations (Reprinted with permission
from Atlas of Infectious Diseases Volume VII: External manifestatins of
systemic infections. Mandel GL, Fekety R, editors. Viral hemorrhagic fevers.
Chapter 10. Peters CJ, Zaki SR, Rollin PE. Churchill-Livingstone. Philidelphia.
1997.

Skin eruptions are uncommon.[44,129] The South American arenaviruses more commonly cause petechiae, purpura, ecchymoses, and palatal hyperemia.
|
|
|
Figures 24a, b: New World Arenavirus-Junin. (a) Conjunctival hemorrhage in a patient with Argentine Hemorrhagic Fever caused by Junin virus. (b) Gingival bleeding in a patient with Argentine Hemorrhagic Fever. (Reprinted with permission from Atlas of Infectious Diseases Volume VII: External manifestatins of systemic infections. Mandel GL, Fekety R, editors. Viral hemorrhagic fevers. Chapter 10. Peters CJ, Zaki SR, Rollin PE. Churchill-Livingstone. Philidelphia. 1997. |
 |
Figure25: Site of Sabia virus infections in Brazil. (Courtesy of Peter B. Jahrling, PhD) |  |
Figure 26: New World Arenavirus-Machupo. Oral mucosal hyperemia and hemorrhage in a patient with Bolivian Hemorrhagic Fever caused by Machupo virus (Photo courtesy of C.J. Peters, M.D.) |
Cutaneous manifestations of HFRS appear on about day three of illness. A petechial rash manifests on the neck, anterior and posterior axillary folds, upper arms, and thorax. A morbilliform eruption may also occur. Flushing may be seen about the head, neck, and upper torso. This may be most apparent in a malar distribution as a ‘sunburn flush’ accompanied by facial edema. Dermatographism is often present. Hemorrhages are often seen on mucosal surfaces and may be severe in the conjunctivae.[9,42,75] Of the other Bunyaviruses, Rift Valley Fever typically causes no skin lesions while CCHF patients generally develop the worst hemorrhagic manifestations
Figure 28: Bunyavirus Infection-CCHF Virus. Ecchymoses
complicating CCHF. (Reprinted with permission
from Atlas of Infectious Diseases Volume VII: External manifestatins of
systemic infections. Mandel GL, Fekety R, editors. Viral hemorrhagic fevers.
Chapter 10. Peters CJ, Zaki SR, Rollin PE. Churchill-Livingstone. Philidelphia.
1997. Figure 29: Apodemus agrarius, the vector of Korean
Hemorrhagic Fever . (Courtesy David McClain, MD) Figure 30: Bunyavirus Infection- Hantaan Virus. Patient
with Korean Hemorrhagic Fever caused by Hantaan virus demonstrating typical
'sunburn flush' of cheeks. (Photo courtesy of John Huggins, PhD.) Figure 31: Bunyavirus Infection. Another patient with
Korean Hemorrhagic Fever demonstrating conjunctival hemorrhages, facial
petechiae, and 'sunburn flush' of cheeks. (Photo courtesy of John Huggins,
PhD.)





Figure 27: Bunyavirus infection- CCHF Virus.
Ecchymoses encompassing left upper extremity one week after onset of CCHF.
Ecchymoses are often accompanied by hemorrhage in other locations: epistaxis,
puncture sites, hematemesis, melena, and hematuria. Reprinted from Jahrling
PB. Viral Hemorrhagic Fevers. Chapter 29 In :Sidell FR, Takafuji ET, Franz
DR, eds., Medical Aspects of Chemical and Biological Warfare. In: Zajtchuk
R, Bellamy RF, eds. Textbook of Military Medicine. Washington, DC: US Department
of the Army, Office of the Surgeon General, and Borden Institute; 1997:595.
Photo courtesy Robert Swaneopoel, PhD, DTVM, MRCVS, National Institute of
Virology, Sandringham, South Africa.
Figure 32: Charcol pit in Kikwit, Zaire
(Democratic republic of the Congo), site of 1995 Ebola fever outbreak. (Courtesy
Peter B. Jahrling, PhD.)
The Filovirus diseases frequently exhibit an exanthem, particularly noted in lighter-skinned patients. Filovirus disease presents with a deep reddening of the soft palate that spreads to the hard palate .
 |
Figure 33: Filovirus disease- Ebola Fever. Patient with Ebola hemorrhagic fever during 1976 outbreak in Zaire demonstrating palatal petechiae and hemorrhage. (Photo courtesy Joel Breman) |
The most reliable diagnostic sign is a pin-head-sized papular, erythematous eruption appearing at days 5-7 on the buttocks, trunk, and lateral arms. After 24 hours, the eruption develops into large, well-demarcated, coalescent macules and papules. In some cases, the rash appears hemorrhagic. In severe cases, a dark, livid erythema develops on the face, trunk, and extremities that disappears in several days. Cyanosis sometimes accompanies the erythema. After the 16th day, palms, soles, dorsal feet, and extremities desquamate for a few days to two weeks. The exanthem is often accompanied by scrotal dermatitis or labial erythema.[89,90]
Like Marburg disease, Ebola fever starts abruptly with fever, myalgias, headache, and other influenza-like symptoms. Early findings include conjunctival injection and adenopathy. Around day 5, a morbilliform eruption followed by petechiae, ecchymoses, and even hemorrhage is seen. Most commonly, the rash is nonpruritic, maculopapular, and centripetal with variable erythema that desquamates by day 7. Patients have expressionless, ghost-like facies. Psychosis, delirium, seizures, and coma are often noted. With progressive disease, hemorrhage exudes from mucous membranes, venipuncture sites, and body orifices. Death occurs between six and 16 days after hemorrhage begins. Mortality rate in pregnancy is 100%.[44,56] Death is due to a combination of hemorrhage, capillary leak, shock due to vasodilatation and hemodynamic deregulation, and end organ failure.[129]
Dengue typically features a morbilliform eruption sparing the palms and soles. Infection due to one of the four serotypes grants lifelong immunity to that serotype only, and predisposes to dengue hemorrhagic fever or dengue shock syndrome following reinfection due to a heterologous strain.[44,132]
|
|
 |
|
Figure 34: Patient with mornilliform exanthem of dengue fever. Note islands of sparing characteristic for dengue. (Photo courtesy Duane Gubler, PhD.) |
Figure 35: Patient with dengue hemorrhagic fever complicated by ecchymoses. (Photo courtesy Duane Gubler, PhD.) |
The only cutaneous manifestation of Yellow Fever is jaundice. The tick-borne Flavivirus diseases (Omsk HF and Kyasanur Forest Disease) can cause any of the hemorrhagic manifestations listed above.
BW Considerations
Hemorrhagic fever viruses cause high morbidity and, in some cases, high mortality. Some may replicate well enough in cell culture to permit weaponization.[105]
Filoviruses could be maliciously adapted as BW agents because they are highly infectious, lethal, and can be stabilized for aerosol dissemination. The Russians experimented with filoviruses as potential BW agents, but apparently discontinued development in the mid-1990s for financial reasons. They successfully enhanced the viability of aerosolized filoviruses.[10] Marburg virus can be stabilized in 10% glycerin so that viral inactivation occurs at a rate of 1.5%/minute instead of 11.5%/minute. This rate of inactivation is in the range of that for influenza virus (1.9%/minute) which spreads naturally by aerosol.[10,59] Filoviruses, however, are considered too dangerous to use because of the lack of protective vaccines and therapeutic measures to protect the users.[2] The Russians evaluated CCHF as a BW agent, but did not weaponize it.[2] The susceptibility of Bunyaviruses to heat, drying, and ultraviolet light make them poor candidates as BW agents.[2] Hantaviruses replicate poorly in cell culture and are not considered to be significant BW threats. The Flaviviridae are unlikely to be used as BW agents. Dengue is not infectious by aerosol, and troops are routinely immunized for yellow fever.
CUTANEOUS COMPLICATIONS OF BW PREVENTION
VIRAL AGENT – Vaccinia
The Orthopox virus vaccinia is distinct from cowpox, has little virulence for immunocompetent humans, and has recently been used as a vector for experimental vaccines.[13] Vaccinia would not be used as a BW agent, but it could cause disease when used to prevent smallpox. The origin of vaccinia is obscure; it may have developed from an extinct animal poxvirus, such as horsepox, or may represent a cowpox mutant, which developed during multiple human passages during the early vaccine era.[125] Smallpox vaccine was prepared (until production stopped in 1983) by inoculating shaved abdomens of calves, sheep, or water buffalo.[114] Infectious exudative lymph was harvested from inoculation sites and bottled with phenol and brilliant green as bacteriostatic agents. Human cell culture-derived vaccinia is being developed at USAMRIID.
Vaccine is administered percutaneously with a bifurcated needle. This process became known as ‘scarification’ because of the resulting permanent scar.[114] Infectious virus replicated in the lesion. It was early determined that vaccinees who received vaccinia by intramuscular injection developed weaker immune responses than those vaccinated by scarification. Scarified patients that develop pox lesions develop 3-fold higher ELISA titers and 10-fold greater plaque reduction neutralization titers than those who develop no pox lesion.[13]
Clinical Response to Vaccination
Primary vaccinees usually developed a pustule surrounded by induration 6-8 days after vaccination. This ‘major reaction’ was required to confer protective immunity and occurred in about 95% of primary vaccinees. All other reactions were termed ‘equivocal.’
|
|
Figure 36: Major reaction to vaccinia consisting of a pustule with surrounding induration. This reaction refleacted active viral replication in the epidermis and the mounting of an immune response by the recipient. (Photo courtesty of David J.McClain, MD) |
The remaining scar was usually about 1 cm in diameter. A rare but severe non-cutaneous side effect of vaccination was post-infectious encephalitis similar to post-measles encephalitis.[15] Vaccinia provides at least three years of protection after vaccination.[127]
 |
Figure 37: Vaccinia: Scar (scarification). (Photo courtesy of James D. Arthur, MD) |
Cutaneous Complications of Vaccinia
Cutaneous complications were at least 10 times more common in primary vaccinees than revaccinees.[118] The most severe cutaneous complication, vaccinia necrosum (vaccinia gangrenosum, progressive vaccinia), occurred in 12.3 per million primary vaccinees.[15,18,126] Vaccinees with cellular immunodeficiencies developed relentlessly progressive pox lesions and even metastatic lesions.[118,128] Fatal cases showed no evidence of resolution, no adenopathy, and no erythema. Death occurred in 13/17 (76%) of documented cases.[127]
|
|
Figures 38a,b: Vaccinia necrosum (progressive vaccinia, vaccinia gangrenosum) represents progressive viral replication in an immunocompromised individual leading to inexorable tissue destruction. Reprinted with permission from Fenner F, Henderson DA, Arita I, Jezek Z, Ladnyi ID. Smallpox and its eradication. Geneva, Switzerland: World Health Organization; 1988:10-14. Photographs byCH Kempe) |
Eczema vaccinatum with hundreds of pox lesions occurred in active atopic dermatitis patients who were vaccinated or merely exposed to a recent vaccinee. Mortality was 10-14%.[15,118] Patients were treated with vaccinia immune globulin 0.6 cc/kg/24 hours until no new lesion appeared.[15] Only 1.5 cases/million primary vaccinees were reported in a U.S. survey.[126] This low rate can likely be explained by the fact that atopic dermatitis was a contraindication to vaccination.[118]
 |
Figure 39: Child with eczema vaccinatum. Reprinted with permission from Fenner F, Henderson DA, Arita I, Jezek Z, Ladnyi ID. Smallpox and its eradication. Geneva, Switzerland: World Health Organization; 1988:298. (Photograph by ID Ladnyi) |
Accidental vaccinia infection occurred among 241.5 per million primary vaccinees by autoinoculation to another body site or to another person (secondary inoculation) via intimate contact (Figure – accidental vaccinia).[126] Ocular vaccinia was one of the most troublesome forms of accidental inoculation.[118]
|
|
Figure 40: Accidental ocular inoculation of vaccinia. Corneal scarring and visual impairment may result. This complication is managed aggressively with topical antiviral drugs. Reprinted with permission from Fenner F, Henderson DA, Arita I, Jezek Z, Ladnyi ID. Smallpox and its eradication. Geneva, Switzerland: World Health Organization; 1988:298. Photographs by CH Kempe) |
Generalized vaccinia is a non-specific term applied to a vesicular eruption developing after primary vaccination. After about 7-12 days, patients developed a rash with many small vesicles on erythematous bases. Patients with generalized vaccinia are non-toxic, afebrile, and not viremic.[15] This self-limited complication generally resolved in 6-9 days in the 38.5 per million primary vaccinees who contracted it.[114,126]
 |
Figure 41: Generalized vaccinia after vaccination. (Fitzsimons Army Medical Center Dermatology Slide File) |
Seven to twelve days after vaccination, some patients develop erythematous urticarial eruptions that resemble enterovirus or roseola exanthems.
Other complications may occur such as melanoma or BCC in vaccination scars. Bullous erythema multiforme, overwhelming and fatal viremia in infants, and fetal vaccinia have also been reported.[15]
AGENTS WITH CUTANEOUS MANIFESTATIONS OF ENDEMIC, BUT NOT BW-ASSOCIATED DISEASE
BACTERIAL AGENT – Bacillus anthracis
Bacillus anthracis is a gram-positive sporulating bacillus. The spores are resistant to heat, cold, drying, and chemical disinfection.[41] Spores remain viable for at least several years (up to 200 years in one study[47]) in the top six cm of soil and in animal products.[26,33,47] Animals that die of anthrax release massive quantities of spores into the soil which may remain for decades before being ingested again. Burying animal carcasses is probably of little use in disrupting transmission since Pasteur showed that earthworms will carry spores back to the surface![41] Animal carcasses should be burned, not buried, to prevent long-term environmental contamination.[61]
Anthrax is endemic in western Asia (Afghanistan, Iran, and Turkey) and western Africa.[26] Disease is transmitted from infected animals or their products via skin abrasions in more than 90% of cases.[27,33,47] Less commonly, ingestion or inhalation of spores transmits anthrax.
|
|
Figure 42: Typical site where cutaneous anthrax is acquired: close proximity to sheep and goats. |  |
Figure 43: Burning rhinocerous carcass after death from anthrax. Burying such an animal will only result in high concentrations of anthrax spores in the soil. |
Clinical Findings
Gastrointestinal (GI) anthrax is exceedingly rare and has never been reported in the U.S.[27] Patients present with ulcerative mucosal eschars that can perforate viscera thus producing abdominal pain, diarrhea, and acute infection. Secondary meningitis has occurred from primary GI disease, but any form of anthrax can progress to septicemia or meningitis.[26,79]
Pulmonary anthrax, or ‘wool-sorter’s disease,’ is an extraordinarily rare form of anthrax; only 18 cases were reported in the U.S. between 1900 and 1980.[27] Anthrax would undoubtedly be used in this form as a BW agent.[105] This usually fatal disease starts as a vague prodrome with fever, malaise, myalgias and cough.[26,27] During the next several days, these non-specific symptoms may be rapidly followed by precordial discomfort, cyanosis, stridor, diaphoresis, moist rales, pleural effusion, and death.[27,41] The initial symptoms mimic any number of influenza-like infections. The disease is difficult to diagnose in the early, treatable stage.[62]
Inhaled spores are engulfed by alveolar macrophages and transported through lymphatics to tracheobronchial lymph nodes within four hours; they replicate in hilar nodes within 18-24 hours. The median lethal inhaled dose is 10,000 spores (range 8000-50,000 spores)[105] that are two to five microns in diameter. The spores can retain viability in the lungs up to 100 days![58] Germination of spores in the hilar nodes leads to hemorrhagic mediastinitis, but not true pneumonia.[62,79] A widened mediastinum on chest X-ray is diagnostically helpful. Overwhelming infection leads to uncontrolled intravascular multiplication of bacilli and fatal toxemia characterized by hypotension and hemorrhage.[62]
Anthrax is generally sensitive to penicillin, however, rare beta-lactamase positive strains have been isolated. Ciprofloxacin, erythromycin, tetracycline, doxycycline, and chloramphenicol are alternative drugs.[62]
Cutaneous Manifestations
 |
 |
| Figure 43a: Cutaneous anthrax on the finger of a veterinarian who contracted condition through animal exposure. Contributed by Robert Aylesworth, M.D. |
Figure 43b: Cutaneous anthrax on the face. As soon as the causitive organism enters the blood stream, an anthrax septicemia results. Reprinted from G. Riehl and Leo V. Zumbusch. Atlas of Diseases of the Skin; Contributed by Rebecca Bushong, M.D. |
Cutaneous disease begins as a small, painless, red macule that progresses to a papule that vesiculates, ruptures, ulcerates, and forms a 1-5 cm[69] diameter brown or black eschar. Lesions usually appear within two weeks after handling sick animals or eating their meat, however, incubation periods of over eight weeks are not unknown.[41,62,68] The black eschar gave rise to the name ‘anthrax’ derived from the Greek word anthrakos meaning ‘coal.’[41,68] Lesions are not purulent in the absence of superinfection.[62] Satellite lesions and significant edema may surround the initial eschar.
Even with prompt antibiotic therapy, cutaneous lesions progress through the eschar phase. Antibiotics have no effect on the skin lesion except to sterilize it.[68] Debridement of skin lesions is contraindicated because of the risk of spreading infection.[26] While 80-90% of lesions heal spontaneously, 10-20% of untreated cases may progress to malignant edema, septicemia, shock, renal failure, and death. Fatalities are uncommon with therapy.[62]
BW Considerations
In a BW scenario, anthrax would most likely be disseminated in aerosol form because the stable spores could cause rapid death in a high percentage of those exposed. In April and May 1979, at least 66 people died during an epidemic of inhalational anthrax in Sverdlovsk, Russia (now Ekaterinburg) following an accidental release of aerosolized spores.[41] All victims had hemorrhagic mediastinitis. It has been estimated that the release of less than one gram of spores caused this outbreak.[63] This accident demonstrated the silent and deadly nature of an aerosol BW attack. Larger quantities of spores released in an urban setting could be an inexpensive and effective terrorist weapon.
Anthrax spores were weaponized by Japan, the United Kingdom, and the United States in the 1940s, 1950s, and 1960s before their offensive programs were terminated. Iraq admitted to a United Nations inspection team in 1995 that they had weaponized anthrax.[105,110]
BACTERIAL AGENT – Francisella tularensis
First described in 1907, Francisella tularensis is a gram-negative, pleomorphic coccobacillus with two serotypes: infection with type A carries a 5% mortality rate while type B causes much milder disease.[34,37] The bacterium can persist for months in mud, water, and decaying animal carcasses, however, it is normally maintained in wild rabbits, squirrels, sheep, beavers, meadow voles, and muskrats.[34,36] Dozens of biting and blood-sucking insects serve as vectors, and ticks pass the bacilli on to offspring trans-ovarially. Dermacentor andersonii (Rocky Mountain wood tick), Dermacentor variabilis (Pacific coast dog tick), and Amblyomma americanum (Lone Star tick) are the main vectors in the United States.[34] Ticks transmit disease during spring and summer in the southwestern and central states while rabbit exposure during the winter accounts for most exposure in southeastern states.[36]
Clinical Findings
Tularemia is highly endemic in Oklahoma, Missouri, and Arkansas.[34] In the decade ending in 1988, 2356 cases were reported in the United States with 24 deaths (1% mortality).[36] Each of the six clinical forms starts with sudden onset of fever, chills, headache, and generalized myalgias and arthralgias after an incubation period of 3-6 days.[114] An ulcer is generally seen at the bite site and may persist several months as organisms spread to local lymph nodes. Untreated, mortality is 8% for all types[34], 4% for ulceroglandular tularemia, and 35% for the typhoidal type.[114] With appropriate treatment, mortality is 1-2.5%.[114] One episode usually guarantees lifelong immunity.[34]
Skin or a mucous membrane acts as the portal of entry for tick bites, other arthropod bites, or abrasions. Rarely, inhaled or ingested organisms cause disease. At least 108 organisms are necessary to cause gastrointestinal disease; only 10 organisms can cause cutaneous or pulmonary infection.[114] Local multiplication of F. tularensis causes a tender, red, pruritic papule that rapidly enlarges to form an ulcer with a black base. The organism then spreads to lymph nodes and causes bacteremia. Conjunctival inoculation leads to local adenopathy. Pneumonia occurs secondary to bacteremia or primarily via aerosolization. Lungs develop foci of alveolar necrosis and neutrophilic infiltrates. Chest x-ray reveals bilateral patchy infiltrates but not large areas of consolidation.[34]
Tularemia classically presents as one of six clinical syndromes:
Ulceroglandular: the most common form of tularemia. With the glandular form, it accounts for 75-85% of naturally occurring cases. The erythematous, indurated, non-healing, punched-out ulcer lasts 1-3 weeks. Local lymph nodes may be fluctuant and drain spontaneously. Suppuration of lymph nodes may occur up to 3 weeks after treatment.[34] The differential diagnosis of ulceroglandular tularemia includes sporotrichosis, cat scratch disease, mononucleosis, lymphangitis, lymphogranuloma venereum, plague, and Pasteurella infections.[36]Glandular: the second most common form. Glandular tularemia follows inoculation of the skin via arthropod vectors and most commonly afflicts the inguinal and femoral lymph nodes in adults and the cervical nodes in children.[34]
Oculoglandular: Inoculation of periorbital skin or the conjunctiva by arthropod vectors or aerosols leads to the development of oculoglandular tularemia.[34]
Oropharyngeal or gastrointestinal: This form follows ingestion of undercooked meat or direct inoculation from the hands to the mouth.[34] Pharyngitis occurs in up to 25% of tularemia patients. The pharynx may be erythematous or may present with petechiae, ecchymoses, ulcers, and/or exudates.[114]
Typhoidal: Only 10-50 organisms need be inhaled to cause typhoidal tularemia. While rare in the United States, it is the septicemic form of disease occurring without skin lesions or lymphadenopathy. One must suspect tularemia to make the diagnosis in time for effective treatment. The disease mortality ranges from 30-60%.[34]
Pulmonary: Pulmonary tularemia develops in 10-30% of those with ulceroglandular disease and in 50-80% of those with typhoidal tularemia.[34,115] Patients present with a non-productive cough with dyspnea or pleuritic chest pain. Chest x-rays reveal a variable parenchymal infiltrate. Up to 30% of patients die.[34] The differential diagnosis includes Q fever, mycoplasma, psittacosis, histoplasmosis, and coccidioidomycosis.[36]
A live-attenuated vaccine is available for individuals at risk (field or laboratory workers) and protects individuals against an aerosol challenge of F. tularensis.[114] Streptomycin is the drug of choice for adults.[114] Gentamicin, tetracycline, ceftriaxone, cefotaxime, chloramphenicol, and ceftazidime are also effective.
Cutaneous Manifestations
A chancre-like ulcer forms at the site of bacterial inoculation in 60% of patients.[114] About 85% of patients develop enlarged lymph nodes[114], some of which present as fluctuant buboes.[116] Mucous membrane lesions in the pharynx commonly accompany aerosol-induced disease.[114] A morbilliform eruption has been reported in a minority of patients with systemic disease.[34]
 |
|
| Figure 44: Ulceroglandular tularemia demonstrating inoculation site on cheek and cervical lymphadenopathy. (Fitzsimons Army Medical Center Dermatology Slide File). |
Figure 45: Typical heaped-up ulcer of tularemia on the scalp. (Reprinted from McGovern TW, Friedlander AM. Plague. In: Sidell FR, Takafuji ET, Franz DR, eds. Medical Aspects of Chemical and Biological Warfare. Chapter 23 In: Zajtchuk R, Bellamy RF, eds. Textbook of Military Medicine. Washington, DC: US Department of the Army, Office of the Surgeon General, and Borden Institute; 1997:505. |
BW Considerations
Tularemia was weaponized by the United States in the 1950s and 1960s. Other countries may have weaponized this agent for delivery by aerosol.[105] Both typhoidal and pulmonary tularemia may result from inhalation of bacilli,[105] and mucous membrane lesions could accompany inhalational disease.[114] The rapid onset of action, non-specific nature of complaints in those affected, and the difficulty in identifying and culturing the organism make it a potential threat agent.[114]
RECOGNIZING A BIOLOGICAL WARFARE ATTACK [91,105]
Because the primary threat from BW agents today is from terrorists, civilians in densely populated regions would be likely targets. Therefore, civilian medical personnel need to be aware of how a BW attack would present to minimize its effects. We cannot presume that such an attack would never happen.[105,106] Fortunately, the United States government has seen the need for increased education. The Federal Emergency Management Agency and local emergency responders and care givers are learning how to recognize and respond to a BW assault.[106]
With current technology, an enemy could complete a BW attack before the local commander or medical officer would know anything had happened. Large and steadily increasing numbers of casualties would present in a shorter period than for a natural epidemic. There may be a large number of rapidly fatal cases with few recognizable signs and symptoms. Multiple diseases could present simultaneously. Vector-borne diseases will appear without natural outbreaks in animals. BW agents would likely have a high attack rate among exposed individuals, and the disease would often be unusual for the geographic area. Because most agents would be delivered in aerosol clouds, many patients would have pulmonary disease caused by agents that don’t usually cause pulmonary disease (anthrax, plague, staphylococcal enterotoxin B).[105,91,5]
Unlike conventional warfare, BW attacks would generally allow time for an effective emergency response to save many lives.[109]
AGENT DOWNWIND REACH (km) DEAD INCAPACITATED Rift Valley Fever 1 400 35,000 Tick-borne encephalitis 1 9500 35,000 Typhus 5 19,000 85,000 Brucellosis 10 500 100,000 Q-fever >20 150 125,000 Tularemia >20 30,000 125,000 Anthrax >20 95,000 125,000
Table 2. Potential BW threat agents, effects and likely routes of exposure. This is not to be construed as an official threat list. Diseases in bold cause cutaneous findings if disease is contracted from aerosol exposure. Underlined diseases cause cutaneous manifestations in endemic disease but not in aerosol-generated disease.
|
Agent Class |
Agent |
Personnel Effect |
Route (BW) |
Skin |
|
Bacterial |
Anthrax |
L |
R |
E |
|
|
Brucellosis |
I |
R, P |
|
|
|
Cholera |
I, L |
G |
|
|
|
Melioidosis |
I, L |
R |
E, BW |
|
|
Plague |
L |
R |
E, BW |
|
|
Q Fever |
I |
R |
|
|
|
Tularemia |
L |
R |
E |
|
Toxins |
Botulinum |
L |
R |
|
|
|
Mycotoxins |
L |
R, G, D |
BW |
|
|
Ricin |
L |
R, G, P |
|
|
|
Staph enterotoxin B |
I |
R, G |
|
|
Viral |
Argentine HF |
I |
R |
E, BW |
|
|
Bolivian HF |
I |
R |
E, BW |
|
|
Congo-Crimean HF |
L |
R |
E, BW |
|
|
Ebola HF |
L |
R |
E, BW |
|
|
Hantaviruses |
I, L |
R |
E, BW |
|
|
Lassa HF |
I, L |
R |
E, BW |
|
|
Marburg HF |
L |
R |
E, BW |
|
|
Rift Valley Fever |
L |
R |
|
|
|
Smallpox |
L |
R |
E, BW |
|
|
Venezuelan Equine Encephalitits ncephEEncephalitis |
I |
R |
|
HF = hemorrhagic fever, L = lethal, I = incapacitating, R = respiratory, G = gastrointestinal, P = percutaneous, D = dermal, E = endemic disease, BW = BW-induced disease
|
.Disease |
Geography |
Source of Human Infection |
Incubation |
|
CCHF Europe |
Africa, Asia |
Tick |
3-12 days |
|
Dengue HF |
Asia, Amer, Africa |
Mosquito |
3-15 days |
|
HFRS |
World-wide |
Rodent |
9-35 days |
|
Junin/Machupo |
X |
Rodent |
7-14 days |
|
KFD |
Omsk India/Russia |
Tick (muskrat-contaminated water) |
3-8 days |
|
Lassa |
Africa |
Rodent, Nosocomial |
5-16 days |
|
Marburg/Ebola |
Africa |
Unknown, Nosocomial |
3-16 days |
|
RVF |
Africa |
Mosquito |
2-5 days |
|
Yellow Fever |
Trop. Africa, S.Am |
Mosquito |
3-15 days |
Bibliography
1. Cieslak T. Introduction to USAMRIID and Overview of
Biological Warfare and Bioterrorism. Course Notes Anonymous1997; 1-8.
2. Jahrling P Anonymous1997; Viral hemorrhagic fevers.
3. Manchee RJ, Stewart WDP. The decontamination of Gruinard Island. Chem Brit
1988; 690-691.
4. Sanford JP. Pseudomonas species (including melioidosis and glanders). In:
Mandell GL, Bennett JE, Dolin R, editors. Principles and practice of infectious
diseases. 4th ed. New York: Churchill Livingston, 1997:2003-2009.
5. McGovern TW, Friedlander A. Plague. In: Sidell FR, Takafuji ET, Franz DR,
editors. Medical Aspects of Chemical and Biological Warfare. . Falls
Church, VA: Office of The Surgeon General, United States Army, 1997:479-502.
6. Butler T. Yersinia species (including plague). In: Mandell GL, Bennett JE,
Dolin R, editors. Principles
and practice of infectious diseases.
4th ed. New York: Churchill Livingston, 1997:2070-2078.
7. Richards CA. Stachybotrys atra suspected in three infant deaths: 18
others sickened. Infectious Diseases in Children 1997; 10:1+-8.
8. Wannemacher RW, Jr., Wiener SL. Trichothecene mycotoxins. In: Sidell FR,
Takafuji ET, Franz DR, editors. Medical Aspects of Chemical and Biological Warfare.
Falls Church, VA: Office of The Surgeon General, United States Army, 1997:655-676.
9. Takami RM. Epidemic hemorrhagic fever. 1951; Medical Section, GHQ, FEC: United
States Army. 1 p.
10. Belanov YF, Muntyanov VP, Kryuk VD, Sokolov AV, Bormotov NI, P'yankov OV,
et al. Retention of Marburg virus infecting capability on contaminated surfaces
and in aerosol particles. Voprosy virusologii 1996; 32-34.
11. Anonymous. WHO sets date to destroy smallpox stocks.
Public Health Reports 1996; 111:388
12. Empson J. Country doctor and speckled monster. Nature
1996; 381:26
13. McClain DJ, Harrison S, Yeager CL, Cruz J, Ennis
FA, Gibbs P, et al. Immunologic responses to vaccinia vaccines administered
by different parenteral routes. J Infect Dis 1997; 175:756-763.
To develop a less reactogenic but equally immunogenic vaccine, this study of 91 human volunteers compared the safety and
immunogenic potency of a new, cell culture-derived vaccinia virus vaccine administered intradermally and intramuscularly with
the licensed vaccinia vaccine administered by scarification. Cutaneous pox lesions developed in a higher proportion of
scarification vaccinees. Scarification and intradermal vaccine recipients who developed cutaneous pox lesions had more local
reactions but also achieved significantly higher cell-mediated and neutralizing antibody responses than those who did not develop
pox lesions. Although less reactogenic, intradermal or intramuscular administration of vaccinia vaccine without the concomitant
development of a cutaneous pox lesion induced lower immune responses.
14. Neff JM. Introduction (Poxviridae). In: Mandell GL, Bennett
JE, Dolin R, editors. Principles and Practice of Infectious Diseases. 4th ed.
New York: Churchill Livingston, 1995:1325
15. Neff JM. Vaccinia virus (cowpox). In: Mandell GL,
Bennett JE, Dolin R, editors. Principles and practice of infectious diseases.
4th ed. New York: Churchill Livingston, 1995:1325-1328
16. Neff JM. Variola (smallpox) and monkeypox viruses.
In: Mandell GL, Bennett JE, Dolin R, editors. Principles and Practice of Infectious
Diseases. 4th ed. New York: Churchill Livingston, 1995:1328-1329.
17. Mwamba PT, Tshioko KF, Moudi A, Mukinda V, Mwema
GN, Messinger D, et al. Human monkeypox - Kasai Oriental, Zaire, 1996-1997.
Morb Mort Wk Rep 1997; 46:304-307.
Monkeypox is an orthopoxvirus with enzootic circulation in rainforests of central and western Africa; the virus can be
transmitted to humans and cause a syndrome clinically similar to smallpox (e.g., pustular rash, fever, respiratory symptoms, and
in some cases, death). From February through August 1996, a total of 71 clinical cases of monkeypox, including six deaths,
occurred in 13 villages in Africa in the Katako-Kombe health zone (1996 combined population: 15,698), Sankuru subregion,
Kasai Oriental, Zaire. During the initial investigation of this cluster of human cases, specimens of serum and/or crusted scab or
fluid from vesicles were collected from 11 patients, and monkeypox virus infection was confirmed in all 11 patients by the World
Health Organization (WHO) Collaborating Center for Smallpox and Other Poxvirus Infections at CDC. Preliminary DNA
phylogenetic studies of this strain of virus indicated only minor genetic variation compared with other strains of monkeypox virus
from Zaire collected during 1970--1979. Because of reports by local public health officials of ongoing disease transmission, the
Zaire Ministry of Health and WHO organized a follow-up investigation in February 1997 to characterize the magnitude of the
outbreak. This report summarizes the preliminary results of the ongoing multidis-ciplinary investigation, which suggest that
person-to-person transmission accounted for most monkeypox cases investigated in 1996 and 1997; in contrast, during previous
years, reports were primarily for sporadic cases that resulted from animal-to-human transmission.
18. Baxby D. Poxviruses. In: Belshe RB, editor. Textbook of
Human Virology. Littleton, MA: PSG Publishing Co. 1984:929-948.
19. Peters W, Gilles HM. Color Atlas of Tropical Medicine
and Parasitology. 4th ed. Barcelona: Mosby-Wolfe, 1995.
20. Immunizations and chemoprophylaxis. 1995; 40-562:
Army Regulation.
21. Anonymous The NIV Study Bible: New International
Version. Grand Rapids: Zondervan Bible Publishers, 1985.
22. Anthrax. 1995;
23. Swartz MN, Weinberg AN. Miscellaneous bacterial infections
with cutaneous manifestations. In: Fitzpatrick TB, Eisen AZ, Wolff K, Freedberg
IM, Austen KF, editors. Dermatology in General Medicine. 4th ed. New York: McGraw-Hill,
1993:2354-2370.
24. Highet AS, Hay RJ, Roberts SOB. Bacterial infections.
In: Champion RH, Burton JL, Ebling FJG, editors. Textbook of dermatology. 5th
ed. Oxford: Blackwell Scientific, 1992:953-1032.
25. Anonymous. Update: Management of patients with suspected
viral hemorrhagic fever - United States. J Am Med Assoc 1995; 274:374-375.
26. Burnett JW. Anthrax. Cutis 1991; 48:113-114.
27. Walker DH, Yampolska O, Grinberg LM. Death at Sverdlovsk:
What have we learned. Am J Pathol 1994; 144:1135-1141.
28. Berthier M, Fauchere J-L, Perrin J, Brignon B, Oriot
D. Fulminant meningitis due to Bacillus anthracis in 11-year-old girl
during Ramadan. Lancet 1996; 347:828
29. Dearborn DG, Smith PG, Brooks LJ, Carroll-Pankhurst
C, Kosick R, Dahms BB. Update: Pulmonary hemorrhage/hemosiderosis among infants
- Cleveland, Ohio, 1993-1996. Morb Mort Wk Rep 1997; 46:33-35.
In November 1994, private physicians and public health officials in Cleveland, Ohio, and CDC reported a cluster of eight cases of
acute pulmonary hemorrhage/ hemosiderosis that had occurred during January 1993--November 1994 among infants in one area
of the city. Two additional cases were identified in December 1994. All 10 infants lived within seven contiguous postal tracts in
eastern metropolitan Cleveland. Pulmonary hemorrhages recurred in five of the infants after they returned to their homes shortly
after hospital discharge; one infant died as a result of pulmonary hemorrhage. This report summarizes the findings of the
follow-up investigation, including a case-control study and an assessment by the county coroner of cases of infant death. These
findings documented an association between acute pulmonary hemorrhage/hemosiderosis in this cluster of cases and mold growth
in their water-damaged homes.
30. Simpson DIH. The filovirus enigma. Lancet 1995; 345:1252-1253.
31. Marwick C. Floods carry potential for toxic mold
disease. J Am Med Assoc 1997; 277:1342
32. Fisher-Hoch SP, Tomori O, Nasidi A, Perez-Oronoz
GI, Fakile Y, Hutwagner L, et al. Review of cases of nosocomial Lassa fever
in Nigeria: the high price of poor medical practice. Brit Med J 1995; 311:857-859.
OBJECTIVE--To investigate two hospital outbreaks of Lassa fever in southern central Nigeria. SETTING--Hospitals and clinics
in urban and rural areas of Imo State, Nigeria. DESIGN--Medical records were reviewed in hospitals and clinics in both areas.
Patients with presumed and laboratory confirmed Lassa fever were identified and contracts traced. Hospital staff, patients, and
local residents were questioned, records were carefully reviewed, and serum samples were taken. Serum samples were assayed
for antibody specific to Lassa virus, and isolates of Lassa virus were obtained. RESULTS--Among 34 patients with Lassa fever,
including 20 patients, six nurses, two surgeons, one physician, and the son of a patient, there were 22 deaths (65% fatality rate).
Eleven cases were laboratory confirmed, five by isolation of virus. Most patients had been exposed in hospitals (attack rate in
patients in one hospital 55%). Both outbreak hospitals were inadequately equipped and staffed, with poor medical practice.
Compelling, indirect evidence revealed that parenteral drug rounds with sharing of syringes, conducted by minimally educated
and supervised staff, fueled the epidemic among patients. Staff were subsequently infected during emergency surgery and while
caring for nosocomially infected patients. CONCLUSION--This outbreak illustrates the high price exacted by the practice of
modern medicine, particularly use of parenteral injections and surgery, without due attention to good medical practice. High
priority must be given to education of medical staff in developing countries and to guidelines for safe operation of clinics and
hospitals. Failure to do so will have far reaching, costly, and ultimately devastating consequences.
33. John TJ. Emerging and re-emerging bacterial pathogens in India. Indian J Med Res 1996; 103:4-18.
In spite of major successes against infectious diseases in the 20th century, new infectious diseases have emerged and old ones
re-emerged in recent decades in different parts of the world. A brief survey of emerging and re-emerging bacterial diseases of
public health importance in India is presented in this paper. Plague re-appeared in two outbreaks in Maharashtra and Gujarat in
1994, indicating a breakdown of the public health measures that had prevented its occurrence for several decades. Leptospirosis
appears to be on the increase in Kerala, Tamilnadu and the Andamans during the last 2 decades, probably due to increased
farming and inadequate rodent control. It is suggested that melioidosis due to the soil organism Burkholderia pseudomallei may
be prevalent in many parts of India, but is under-diagnosed and under-reported. Since 1991, a completely new choleragenic
Vibrio cholerae, designated 0139 has emerged in southern India and spread to other parts of India and to neighbouring countries,
setting in motion the 8th cholera pandemic. Animal anthrax is very common in many parts of India, but human anthrax is
recognised in only certain limited locations. In the Chittoor and North Arcot districts, its prevalence had increased in recent
years. Since 1990, a multi-drug resistant variety of typhoid fever had been prevalent in many parts of India, caused by Salmonella
typhi resistant to chloramphenicol, ampicillin and trimethoprim-sulphamethoxazole. Nosocomial methicillin-resistant
Staphylococcus aureus infection seems to be widely prevalent in hospitals in many regions in India, and its prevalence seems to
be on the rise. These pathogens pose new threats to public health, and call for appropriate responses. Microbiological expertise
and epidemiological surveillance are deficient in the health care and public health systems in India; therefore even infections and
diseases that have been under control elsewhere remain prevalent in the country, but are also under-diagnosed and
under-reported. Without improving microbiological expertise and application as well as epidemiological skills and practices,
emerging and re-emerging diseases may not be recognised, identified or intercepted in their early stages.
34. Jacobs RF. Tularemia. Adv Pediatr Infect Dis 1996; 12:55-69.
35. Walker DH, Barbour AG, Oliver JH, Lane RS, Durnier
S, Dennis DT, et al. Emerging bacterial zoonotic and vector-borne diseases.
J Am Med Assoc 1996; 275:463-369.
Among the etiologic agents of emerging infectious diseases are several bacterial organisms that naturally reside in animal and
arthropod hosts. The most compelling emerging bacterial zoonotic and vector-borne diseases in the United States are Lyme
disease; a Southern erythema migrans-like illness; human monocytic ehrlichiosis; human granulocytic ehrlichiosis; a novel cat
flea-associated typhus group rickettsiosis; bartonelloses of immunocompetent and immunocompromised persons, particularly
with AIDS; and sylvatic plague. Some of these antimicrobial-treatable infections are life threatening. During the acute stage of
illness when antimicrobial agents are most effective, the flulike clinical signs and symptoms and available laboratory tests
frequently do not point to a particular diagnosis. Epidemiological factors determined by the ecology of the bacteria are often the
most useful diagnostic clues. The recognition of these evolving problems emphasizes the need for development of better
laboratory diagnostic methods, for surveillance for and tracking of disease, and for continued research into factors contributing to
transmission of the organisms. The continual appearance of previously unidentified bacterial infections requires prospective
national strategies for timely recognition of the syndrome, identification of the agent, establishment of criteria and methods for
diagnosis, optimization of the treatment regimen, and determination of successful approaches to prevention and control.
36. Langley R, Campbell R. Tularemia in North Carolina, 1965-1990.
N Carolina Med J 1995; 56:314-317.
37. U.S.Department of Health and Human Services, Public
Health Service, Centers for Disease Control and Prevention, National Institutes
of Health. Biosafety in microbiological and biomedical laboratories. HHS Publication
No (CDC) 93-8395 Anonymous1993; 3rd Edition:
38. Anonymous. Zoonoses control. Weekly Epidemiol Rec
1996; 71:371-373.
39. Aronson SM. An old diagnostic test for plague. Med
Health Rhode Island 1996; 79:349-350.
40. Katz AM. Nasal anthrax in Boston. Pharos 1995; 58:48-49.
41. Farrar WE. Anthrax: from Mesopotamia to molecular
biology. Pharos 1995; 58:35-38.
42. Hart CA, Bennett M. Hantavirus: an increasing problem.
Ann Trop Med Parasitol 1994; 88:347-358.
Hantaviruses are enveloped RNA viruses and members of the Bunyaviridae family. They are transmitted from various rodent
hosts by inhalation of infected urine, saliva or faeces. Infection in rodent hosts is inapparent but persists for life. Person-to-person
spread of hantavirus has not been described. Two main presentations of the disease occur. Haemorrhagic fever with renal
syndrome (HFRS) is due to Hantaan, Seoul, Puumala, Porogia and Belgrade viruses. In general HFRS due to Hantaan, Porogia
and Belgrade viruses is more severe and has higher mortality than that due to Puumala (nephropathia epidemica) or Seoul
viruses. Hantaan is predominant in the Far East (Korea, Japan, China), Porogia and Belgrade in the Balkans, and Puumala in
Western Europe; Seoul has a world-wide distribution. Hantavirus pulmonary syndrome (HPS) is a recently described infection
with high mortality (60%) due to adult respiratory distress syndrome. The virus (Muerto Canyon Virus) is a hantavirus but
different genotypically from previous strains. Management of hantavirus infections may require bed-rest, sedation, circulatory
and ventilatory support and renal dialysis. Ribavirin if administered early in the illness may be of benefit.
43. Walsh AL, Wuthiekanun V. The laboratory diagnosis of melioidosis. Br J Biomed Sci 1996; 53:249-253.
The recognition of unusual, but important, pathogens such as Burkholderia pseudomallei is essential for the rapid implementation
of appropriate antimicrobial therapy--delays can be fatal. Melioidosis should be considered as a potential diagnosis for any
patient with exposure to areas of endemicity, and thus laboratories should be aware of the differential features of the disease and
the causative organism. Isolation of B. pseudomallei is readily achieved using standard culture media such as blood, MacConkey
or cystine-lactose-electrolyte-deficient (CLED) agars, and routine blood culture broths. Selective media, Ashdown's agar and
selective broth, are required for respiratory tract specimens to ensure reliable isolation from amongst the normal or contaminating
flora. These media are easily prepared from common media constituents. Colonial morphology and simple biochemical tests will
suggest the identity of the organism, which can then be confirmed by additional tests for 'non-fermenters', such as the API 20NE.
44. Lacy MD, Smego RA. Viral hemorrhagic fevers. Adv Pediatr
Infect Dis 1996; 12:21-53.
45. Handa R, Bhatia S, Wali JP. Melioidosis: a rare but
not forgotten cause of fever of unknown origin. Br J Clin Pract 1996; 50:116-117.
Melioidosis is widely prevalent in Southeast Asia and northern Australia. Although it is believed to pose no current threat to the
populations of developed countries, the increased mobility of people around the world and of Southeast Asian refugees to
Western countries may change this. Its long incubation period may put a relatively large number of currently asymptomatic
people at risk. It should be considered in the differential diagnosis of any febrile illness in a person who has visited an endemic
area, especially if the presenting features are those of fulminant respiratory failure, if multiple pustular or necrotic skin or
subcutaneous lesions develop, or if there is a radiologic pattern of tuberculosis from which tubercle bacilli cannot be
demonstrated.
46. Yap EH, Thong.T.W., Tan AL, Yeo M, Tan HC, Loh H, et al. Comparison of Pseudomonas pseudomallei from humans, animals, soil and water by restriction endonuclease analysis. Singapore Med J 1995; 36:60-62.
Pseudomonas pseudomallei isolates from 62 human, 17 animal, 3 soil and 3 water samples were examined by genomic DNA
digestion with PstI. Five major (RE I, II, III, IV, V) reproducible restriction patterns were observed, with most (56/62) of the
human isolates displaying RE I (30/62), II (5/62), III (15/62), IV (4/62), V (2/62), and the animal (16/17), soil (2/3), water (3/3)
isolates showing predominantly RE II profiles. Six human and one soil isolates showed patterns different from those of RE I to V.
Restriction endonuclease analysis may be applied in epidemiological studies of melioidosis.
47. Titball RW, Turnbull PCB, Hutson RA. The monitoring and
detection of Bacillus anthracis in the environment. J Appl Bacteriol
Symp 1991; 70:9S-18S.
48. Cherian T, John TJ, Ramakrishna B, Lalitha MK, Raghupathy
P. Disseminated melioidosis. Indian Pediatr 1996; 33:403-406.
49. Anonymous. British soldier returns from Bosnia with
HFRS. Communicable Disease Report 1996; 5:193
50. Tukei PM. Threat of Marburg and Ebola viral haemorrhagic
fevers in Africa. East Afr Med J 1996; 73:27-31.
Marburg and Ebola viruses are members of the filovirus family that can be regarded as recently emerged. These viruses have
caused sporadic outbreaks of fatal haemorrhagic disease in Africa, Europe and recently in the USA. The case fatality rates rank
among the highest ranging from 33-80%. The mode of transmission of these viruses are clearly through close contact with blood
and body fluids. Disease outbreaks have been amplified in hospital situations with poor blood precautions. In villages disease has
been amplified through contamination with blood and fluids during nursing the sick and burial rituals. The source of the viruses
has eluded discovery and new theories regarding the nature of these viruses are being entertained. The threat of new outbreaks in
Africa is real since serological evidence of the presence of the virus has been documented in Kenya, Sudan, Zaire, Zimbabwe,
Gabon, Cote-d'Ivoire and Gabon.
51. Healing TD, Hoffman PN, Young SEJ. The infection hazards of human cadavers. Communicable Disease Report 1995; 5:R61-R68.
Cadavers may pose infection hazards to people who handle them. None of the organisms that caused mass death in the past--for
example, plague, cholera, typhoid, tuberculosis, anthrax, smallpox--is likely to survive long in buried human remains. Items such
as mould spores or lead dust are much greater risks to those involved in exhumations. Infectious conditions and pathogens in the
recently deceased that present particular risks include tuberculosis, group A streptococcal infection, gastrointestinal organisms,
the agents that cause transmissible spongiform encephalopathies (such as Creutzfeldt-Jakob disease), hepatitis B and C viruses,
HIV, and possibly meningitis and septicaemia (especially meningococcal). The use of appropriate protective clothing and the
observance of Control of Substances Hazardous to Health regulations, will protect all who handle cadavers against infectious
hazards.
52. Steyn PS. Mycotoxins, general view, chemistry, structure. Toxicol Lett 1995; 82/83:843-851.
Mycotoxins induce diverse and powerful biological effects in test systems; some are carcinogenic, mutagenic, teratogenic,
estrogenic, hemorrhagic, immunotoxic, nephrotoxic, hepatotoxic, dermotoxic, and neurotoxic. Mycotoxins have been
unambiguously linked to the etiology of several diseases in animals. The discovery of aflatoxins in the early 1960s led to the
resurgence of interest in human mycotoxicoses; mycotoxins are now recognized as causal factors of primary liver cancer,
ergotism and alimentary toxic aleukia. The fumonisins and ochratoxins are suspected of playing a role in the etiology of
esophageal cancer and Balkan endemic nephrotoxicity, respectively.
53. Neal GE. Genetic implications in the metabolism and toxicity of mycotoxins. Toxicol Lett 1995; 82/83:861-867.
In common with many xenobiotics, metabolic activation and detoxification play crucial roles in the determination of a toxic
response of animal species, including man, to exposure to mycotoxins. Control of expression of the relevant enzymes, both
constitutive and inducible, is therefore a major factor in mycotoxin-induced acute or chronic toxicities. The involvement of these
factors in the toxic responses to aflatoxins and ochratoxins will be briefly reviewed. In the case of the aflatoxins, the importance
of secondary, conjugating metabolism has become increasingly evident. The specific control of expression of these enzymes,
through sequences present in the 5' region of the gene, is evident (e.g. by the changes seen during development and differences
between the sexes). The existence of these control mechanisms has made feasible the development of chemoprotective strategies.
Although less detailed information is available concerning the metabolic activation and detoxification of the ochratoxins, it
appears probable that future studies will reveal a role for the genetic control of expression of enzymes responsible for the target
nephrotoxicity of these mycotoxins.
54. McKenna P, Clement J, Matthys P, Coyle PV, McCaughey C. Serological evidence of hantavirus disease in Northern Ireland. J Med Virol 1994; 43:33-38.
Since, to our knowledge, no clinically documented cases of haemorrhagic fever with renal syndrome (HFRS) have been reported
in Northern Ireland, a sero-epidemiological study was carried out to assess the degree of Hantavirus immunity in a group of 627
Northern Irish patients presenting with symptoms suggestive of HFRS and 100 healthy controls. IFA screening for IgG
Hantavirus specific antibodies was carried out with a panel of up to 9 different Hantaviral antigens. IgM screening was
performed using a commercially available mu-capture ELISA based upon two recombinant Hantaviral nucleocapsid antigens. A
seropositivity of 2.1% (15/727) was recorded, with an almost exclusive reaction against a rat-derived R22VP30 strain of the
Seoul serotype. Sole reliance upon non-rat-derived classic screening antigens Hantaan (HTN 76-118) and Puumala (CG 18-20)
would have resulted in the detection of only 2/15 (13.3%) of cases in IgG IFA, and 8/14 (57.1%) of the cases in IgG ELISA. The
findings indicate that for the first time in Europe, and more specifically in N. Ireland, non-laboratory outbreaks of HFRS may be
caused by wild rats acting as a reservoir for a Seoul-like Hantavirus. Conventional Hantavirus serology using Hantaan and
Puumala as screening antigens does not appear sufficient for the detection of such cases of HFRS. Hence, we propose the
addition of a rat derived Hantaviral antigen to the antigen screening panel as a means of improving the specificity of the
detection methods.
55. Ivins B, Fellows P, Pitt L, Estep J, Farchaus J, Friedlander A, et al. Experimental anthrax vaccines: efficacy of adjuvants combined with protective antigen against an aerosol Bacillus anthracis spore challenge in guinea pigs. Vaccine 1995; 13:1779-1784.
The efficacy of several human anthrax vaccine candidates comprised of different adjuvants together with Bacillus anthracis
protective antigen (PA) was evaluated in guinea pigs challenged by an aerosol of virulent B. anthracis spores. The most
efficacious vaccines tested were formulated with PA plus monophosphoryl lipid A (MPL) in a squalene/lecithin/Tween 80
emulsion (SLT) and PA plus the saponin QS-21. The PA+MPL in SLT vaccine, which was lyophilized and then reconstituted
before use, demonstrated strong protective immunogenicity, even after storage for 2 years at 4 degrees C. The MPL component
was required for maximum efficacy of the vaccine. Eliminating lyophilization of the vaccine did not diminish its protective
efficacy. No significant alteration in efficacy was observed when PA was dialyzed against different buffers before preparation of
vaccine. PA+MPL in SLT proved superior in efficacy to the licensed United States human anthrax vaccine in the guinea pig
model.
56. Feldmann H, Klenk H. Marburg and Ebola viruses. Adv Virus
Res 1996; 47:1-52.
57. Perry RD, Fetherston JD. Yersinia pestis -
Etiologic agent of plague. Clin Microbiol Rev 1997; 10:35-66.
Plague is a widespread zoonotic disease that is caused by Yersinia pestis and has had devastating effects on the human
population throughout history. Disappearance of the disease is unlikely due to the wide range of mammalian hosts and their
attendant fleas. The flea/rodent life cycle of Y. pestis, a gram-negative obligate pathogen, exposes it to very different
environmental conditions and has resulted in some novel traits facilitating transmission and infection. Studies characterizing
virulence determinants of Y. pestis have identified novel mechanisms for overcoming host defenses. Regulatory systems
controlling the expression of some of these virulence factors have proven quite complex. These areas of research have provide
new insights into the host-parasite relationship. This review will update our present understanding of the history, etiology,
epidemiology, clinical aspects, and public health issues of plague.
58. Friedlander AM, Welkos SL, Pitt MLM, Ezzell JW, Worsham PL, Rose KJ, et al. Postexposure prophylaxis against experimental inhlalation anthrax. J Infect Dis 1993; 167:1239-1242.
Inhalation anthrax is a rare disease that is almost invariably fatal. This study determined whether a prolonged course of
postexposure antibiotics with or without vaccination would protect monkeys exposed to a lethal aerosol dose of Bacillus
anthracis when the antibiotic was discontinued. Beginning 1 day after exposure, groups of 10 animals were given penicillin,
ciprofloxacin, doxycycline, doxycycline plus vaccination, vaccination alone, or saline. Antibiotics were administered for 30 days
and then discontinued. Vaccine was given on days 1 and 15. Two animals died of causes other than anthrax and were not
included in the statistical analysis. Nine of 10 controls and 8 of 10 animals given only vaccine died. Each antibiotic regimen
completely protected animals while on therapy and provided significant long-term protection upon discontinuance of the drug
(penicillin, 7 of 10 survived, P < .02; ciprofloxacin, 8 of 9 survived, P < .002; doxycycline, 9 of 10 survived, P < .002;
doxycycline plus vaccination, 9 of 9 survived, P < .0002). Protection against rechallenge was provided by combining
postexposure antibiotic treatment with vaccination.
59. Speed BR, Gerrard MP, Kennett ML, Catton MG, Harvey BM. Viral haemorrhagic fevers: current status, future threats. Med J Australia 1996; 164:79-83.
In developing countries, the major outbreaks of viral haemorrhagic fevers such as Marburg, Ebola and Lassa fever viruses have
been nosocomially spread. The high mortality and absence of specific treatment have had a devastating effect. Epidemics of this
highly contagious disease remain a constant threat to Australia and, as a result, carefully planned laboratory and public health
strategies and clinical infection control measures have been instituted for the management of suspected cases.
60. Kant S, Nath LM. Control and prevention of human plague.
Indian J Pediatr 1994; 61:629-633.
61. Anonymous. Anthrax control and research, with special
reference to national programme development in Africa: Memorandum from a WHO
meeting. Bull W H O 1994; 72:13-22.
The prevalence of anthrax in both animal and human populations has been increasing in Africa. It was therefore appropriate for
this WHO meeting to be convened in an endemic area of the Western Province of Zambia in 1992. The participants reviewed
anthrax epidemiology and control in some African countries, elaborated national anthrax control and research programmes in
Africa, discussed international cooperation and work plans, and elaborated recommendations for anthrax control in Africa. The
discussions centred on anthrax surveillance and reporting systems, diagnosis, vaccine production and immunization, disinfection
and decontamination, carcass disposal, treatment of human cases, health systems, as well as intersectorial cooperation between
public health services, veterinary services and other services such as wildlife conservation, so that national control programmes
could take full account of the conditions prevailing in epidemic situations in Africa. The recommendations are applicable in other
regions where anthrax poses similar problems in public, animal and environmental health.
62. LaForce FM. Anthrax. Clin Infect Dis 1994; 19:1009-1014.
63. Meselson M, Guillemin J, Hugh-Jones M, Langmuir A,
Popova I, Shelokov A, et al. The Sverdlovsk anthrax outbreak of 1979. Science
1994; 266:1202-1208.
In April and May 1979, an unusual anthrax epidemic occurred in Sverdlovsk, Union of Soviet Socialist Republics. Soviet officials
attributed it to consumption of contaminated meat. U.S. agencies attributed it to inhalation of spores accidentally released at a
military microbiology facility in the city. Epidemiological data show that most victims worked or lived in a narrow zone
extending from the military facility to the southern city limit. Farther south, livestock died of anthrax along the zone's extended
axis. The zone paralleled the northerly wind that prevailed shortly before the outbreak. It is concluded that the escape of an
aerosol of anthrax pathogen at the military facility caused the outbreak.
64. Mohan A, Misra A. Use of face masks during a plague epidemic.
Postgrad Med J 1996; 72:127
65. Frean JA, Arntzen L, Capper T, Bryskier A, Klugman
KP. In vitro activities of 14 antibiotics against 100 human isolates of Yersinia
pestis from a Southern African plague focus. Antimicrobial Agents Chemother
1996; 40:2646-2647.
A limited repertoire of antimicrobial agents is currently in use for the treatment of plague. We investigated the in vitro activities
of some newer antimicrobial agents against Yersinia pestis. Among the injectable agents tested, cefotaxime was the most active,
and among the oral agents, both levofloxacin and ofloxacin were highly active, with MICs at which 90% of isolates are inhibited
of < 0.03 microgram/ml. the susceptibilities to the ketolide RU004 and the penem faropenem warrant attention. The enhanced
activities of quinolones against Y. pestis suggest that these agents should be further investigated for the treatment of human
plague in the future.
66. Anonymous. Acting against anthrax: US military veterinarian
helps Haitians and their animals. J Am Vet Med Assoc 1995; 207:1533-1535.
67. Pinner RW. Addressing the challenges of emerging
infectious diseases. Am J Med Sci 1996; 311:3-8.
Through the recent examples of diphtheria in the former Soviet Union, plague in India, and trends in pneumonia mortality in the
United States, the author, in this article, illustrates issues in emerging infectious diseases. The Centers for Disease Control's plan,
Addressing Emerging Infectious Disease Threats: A Prevention Strategy for the United States, is summarized. Initial efforts to
implement this plan are described, with particular focus on the development of Emerging Infections Programs, which are
conducting epidemiologic and laboratory projects on several infectious diseases, including invasive bacterial diseases,
unexplained deaths, foodborne diseases, and ehrlichiosis in four population-based sites in the United States.
68. Singh RSJ, Sridhar MS, Sekhar PC, Bhaskar CJ. Cutaneous anthrax - a report of ten cases. J Assoc Phys India 1992; 40:46-49.
The clinical features of ten cases of cutaneous anthrax are reported. Six males and four females were affected. Their ages ranged
from one and a half year to sixty years. The average incubation period was 8 days. Fever and headache were common systemic
manifestations. Pruritus and ulcer with formation of black eschar were typical features. The patients were treated with penicillins
and chloramphenicol. There was no mortality. Possible human-to-human spread in a patient is discussed.
69. Lakshmi N, Kumar AG. An epidemic of human anthrax - a study. Indian J Pathol Microbiol 1992; 35:1-4.
Twenty-five cases of human anthrax, occurring after contact with a Jercy cow infected with B. anthracis and consumption of its
improperly cooked meat after death, were reported. Cutaneous anthrax was the predominant variety in 18 persons, 7 had
intestinal anthrax, out of them 2 children died, 5 adults survived and one among them developed associated cutaneous anthrax
also. All the persons with cutaneous anthrax recovered with treatment.
70. Hirota K, Wake A. Pathology of Pestis minor. Contrib
Microbiol Immunol 1995; 13:267-272.
71. Alexeyev OA, Morozov VG, Suzdaltseva TV, Mishukov
AS, Steinberg LA. Impaired neturophil function in the cutaneous form of anthrax.
Infection 1994; 4:281-282.
Spontaneous and Bacillus anthracis induced luminol-dependent chemiluminescence of neutrophils was studied in six patients
with the cutaneous form of anthrax. Spontaneous chemiluminescence in anthrax was decreased compared to the healthy controls
(p < 0.05). B. anthracis, opsonized by complement-containing sera from patients, induced chemiluminescence in neutrophils
from control donors but not from patients. B. anthracis, opsonized by complement-free sera from the patients, did not cause an
increase in chemiluminescence response in either the patient or the control neutrophils. Also, B. anthracis, opsonized with normal
sera and nonopsonized, did not induce chemiluminescence in either patient or control neutrophils. It was concluded that
oxidative metabolism by neutrophils is impaired in anthrax, whereas the functional capacity of antibodies seems to be
unaffected.
72. Baxby D, Bennett M, Getty B. Human cowpox 1969-93: a review of 54 cases. Br J Dermatol 1994; 131:598-607.
This survey of the clinical and epidemiological features of human cowpox, a rare but relatively severe zoonotic infection, is
based on 54 cases, many unpublished, which we have studied since 1969. Patients present with painful, haemorrhagic pustules or
black eschars, usually on the hand or face, accompanied by oedema, erythema, lymphadenopathy, and systemic involvement.
Severe, occasionally fatal, cases occur in eczematous and immunosuppressed individuals, although cowpox has not yet been
reported in anyone infected with the human immunodeficiency virus. Variations in the clinical features are described, and the
differential clinical diagnosis of cowpox, parapox, herpes virus, and anthrax infections is discussed. The role of the laboratory in
diagnosis is described, and the value of electron microscopy in providing rapid confirmation is emphasized. Care in taking a
detailed history will assist in the initial clinical diagnosis, and a history of contact with domestic cats, particularly during
July-October, is important. The possible influence of smallpox vaccination on the incidence and severity is discussed and
discounted.
73. Doll JM, Zeitz PS, Ettestad P, Bucholtz AL, Davis T, Gage K. Cat-transmitted fatal pneumonic plague in a person who traveled from Colorado to Arizona. Am J Trop Med Hyg 1994; 51:109-114.
Plague, primarily a disease of rodents and their infected fleas, is fatal in 50% of infected humans if untreated. In the United
States, human cases have been concentrated in the southwest. The most common modes of plague transmission are through flea
bites or through contact with infected blood or tissues; however, primary pneumonic plague acquired from cats has become
increasingly recognized. We report on the case investigation of a patient, presumably exposed to a plague-infected cat in
Colorado, who presented with gastrointestinal symptoms, and subsequently died of primary pneumonic plague. Public health
officials should be vigilant for plague activity in rodent populations, veterinarians should suspect feline plague in ill or deceased
cats, and physicians should have a high index of suspicion for plague in any person who has traveled to plague enzootic areas.
74. Huxsoll DL. Narrowing the zone of uncertainty between research and development in biological warfare defense. Ann N Y Acad Sci 1992; 666:177-190.
Although "research" is not prohibited by the Biological Weapons Convention, States Parties to the Convention have maintained
the spirit of the Convention in actions relating to research. The confidence-building measures agreed to at RC2 refer to research
facilities, publication of research results, and promotion of contacts between scientists engaged in research related to the
Convention. However, assessment of basic research on biological agents is not a productive way to distinguish an offensive from
a defensive program. Additionally, if a country were to initiate a biological weapons program, basic research on biological agents
may not be necessary. For example, the extensive published research on Bacillus anthracis, both as a cause of anthrax in cattle
and other species and as a biological-warfare agent, would enable any motivated group or nation to initiate a biological weapons
program that could immediately advance to the development and scale-up stages. Research on biological agents for offensive
purposes would be characterized by activities such as selection for growth, virulence, and toxin production; improving stability
under varying environmental conditions; and selection of strains that might overcome existing means of prophylaxis and
treatment. A biological program with an offensive intent would in most cases be characterized by evidence of development
efforts in mass production and dissemination, which are often agent-specific. Thus, an assessment of development may
distinguish offensive from defensive programs. If a country were to initiate a biological weapons research program, and were
willing to risk worldwide condemnation should existence of such a program become known, it is likely that such a program would
include development and production capabilities. If a country were not committed to production capability, there would be no
rationale for an offensive biological research that would bring worldwide condemnation. Critics of the U.S. Biological Defense
Research Program have suggested that the program could easily and quickly be turned into an offensive effort. To accomplish
this, however, we have to assume that all military personnel, including the civilians employed by the Department of the Army,
are unethical and willing to break the law and run the risk of placing the U.S. in a noncompliance status. The Army is under
constant scrutiny by governmental agencies, by visiting scientists, by audiences at scientific meetings, by scientists who review
manuscripts for publications, by news media, and by private citizens.
75. Hjelle B, Jenison SA, Goade DE, Green WB, Feddersen RM, Scott AA. Hantaviruses: clinical, microbiologic, and epidemiologic aspects. Crit Rev Clin Lab Sci 1995; 32:469-508.
Hantaviruses comprise a genus of the family Bunyaviridae. Bunyaviruses are enveloped viruses with a negative-sense, tripartite
RNA genome. Hantaviruses are etiologic agents for two acute and severe illnesses of man, hemorrhagic fever with renal
syndrome (HFRS) and hantavirus pulmonary syndrome (HPS). Each hantavirus is primarily associated with a single rodent host
species or genus, and is transmitted to man through accidental inhalation or ingestion of virus-contaminated rodent excreta. The
distribution of hantaviruses is worldwide. HFRS is caused by infection with Hantaan, Seoul, Dobrava/Belgrade, and Puumala
hantaviruses, all of which are enzootic in murid rodents of Old World origin. HPS is caused by any of several hantavirus species
associated with indigenous New World rodents of the subfamily Sigmodontinae, family Muridae. HFRS and HPS have numerous
common epidemiologic, clinical, and laboratory characteristics. Common features include fever, myalgia, thrombocytopenia,
neutrophilia, and a profound capillary leak syndrome associated with hypotension, decreased cardiac output, and shock.
Worldwide, HPS is much less common than HFRS but is associated with a higher mortality rate. Recovery from hantavirus
disease is generally complete, although chronic renal insufficiency may be a rare sequel of HFRS.
76. Glass GE, Watson AJ, LeDuc JW, Childs JE. Domestic cases
of hemorrhagic fever with renal syndrome in the United States. Nehpron 1994;
68:48-51
77. Chaowagul W. Melioidosis; a treatment challenge.
Scand J Infect Dis Suppl 1996; 101:14-16.
78. McCarthy MC, Haberberger RL, Salib AW, Soliman BA,
El-Tigani A, Khalid IO, et al. Evaluation fo arthropod-borne viruses and other
infectious disease pathogens as the causes of febrile illnesses in the Khartoum
province of Sudan. J Med Virol 1996; 48:141-146.
79. Abramova FA, Grinberg LM,
Yampolskaya O, Walker DH. Pathology of inhalational anthrax in 42 cases from
the Sverdlovsk outbreak of 1979. Proc Natl Acad Sci USA 1993; 90:2291-2294.
80. Jayaraman KS. Indian confirms identity of plague.
Nature 1995; 373:65.
81. Bonacorsi SP, Scavizzi MR, Guiyoule A, Amouroux JH,
Carniel E. Assessment of a fluorquinolone, thre betaj-lactams, two aminoglycosides,
and a cycline in treatment of murine Yersinia pestis infection. Antimicrobial
Agents Chemother 1994; 38:481-486.
82. Ip M, Osterberg LG, Chau PY, Raffin TA. Pulmonary
melioidosis. Chest 1995; 108:1420-1424.
83. Lewis-Jones MS, Baxby D, Cefai C, Hart CA. Cowpox
can mimic anthrax. Br J Dermatol 1993; 129:625-627.
84. Feldmann H, Slenczka W, Klenk H. Emerging and reemerging
of filoviruses. Arch Virol 1996; 11:77-100.
85. Anonymous. Human plague in 1994. Weekly Epidemiol
Rec 1996; 71:165-168.
86. Anonymous. Lassa fever. Weekly Epidemiol Rec 1996;
71:194.
87. Bhat RV. Aflatoxin and liver injury. Trop Gastroenterol
1996; 17:153-160.
88. Auwaerter PG, Oldach D, Munday LM, Burton A, Warner
ML, Vance E, et al. Hantavirus serologies in patients hospitalized with community-acquired
pneumonia. J Infect Dis 1996; 173:237-239.
89. Martini GA. Marburg virus disease. Clinical syndrome.
In: Martini GA, Siegert R, editors. Marburg virus disease. New York: Springer-Verlag,
1971:1-9.
90. Stille W, Bohle E. Clinical course and prognosis
of Marburg virus ("Green-Monkey") disease. In: Martini GA, Siegert R, editors.
Marburg virus disease. New York: Springer-Verlag, 1971:10-18.
91. North Atlantic Treaty Organization. NATO handbook
on the medical aspects of NBC defensive operations. Part II - Biological. NATO
Amed P-6(B) Anonymous1996;
92. Christopher GW, Cieslak TJ, Pavlin JA, Eitzen EM,
Jr. Biological Warfare: A Historical Perspective. J Am Med Assoc 1997; 278:412-417.
93. Steck WD, Byrd RB. Urticaria secondary to pulmonary
melioidosis.Report of a case. Arch Dermatol 1969; 99:80-81.
94. Welty TK. Plague. Am Fam Phys 1986; 33:159-164.
95. Mee C. How a mysterious disease laid low Europe's
masses. Smithsonian 1990; 20:66-79.
96. Legters LJ, Cottingham AJ, Jr., Hunter DH. Clinical
and epidemiologic notes on a defined outbreak of plague in Vietnam. Am J Trop
Med Hyg 1970; 19:639-652.
97. Williams P, Wallace D. Unit 731: Japan's secret biological
warfare in World War II. New York: The Free Press, 1989.
98. Haig AM, Jr. Chemical warfare in Southeast Asia and
Afghanistan: Report to congress from secretary of state Alexander M. Haig, Jr.
Special Report No 98 Anonymous1982;
99. Bunner DL, Upshall DG, Bhatti AR. Toxicology data
on T-2 toxin. Report of focus officers meeting on Mycotoxin Toxicity Anonymous1985;
100. Wannemacher RW, Jr., Bunner DL, Neufeld HA. Toxicity
of trichothecenes and other related mycotoxins in laboratory animals. In: Smith
JE, Hendeson RS, editors. Mycotoxins and animal foods. Boca Raton, FL: CRC Press,
1991:499-552.
101. Buck GM, Flowerree CC. International handbook on
chemical weapons proliferation. New York: Greenwood Press, 1991.
102. Crook LD, Tempest B. Plague: A clinical review of
27 cases. Arch Int Med 1992; 152:1253-1256.
103. Welty TK, Grabman J, Kompare E. Nineteen cases of
plague in Arizona: A spectrum including ecthyma gangrenosum due to plague and
plague in pregnancy. Western J Med 1985; 142:641-646.
104. Anonymous. Proliferation of weapons of mass destruction:
Assessing the risk. <None Specified> Anonymous1993; OTA ISC 559:
105. Franz DR, Jahrling PB, Friedlander AM, McClain DJ,
Hoover DL, Byrne WR, et al. Clinical recognition and management of patients
exposed to biological warfare agents. J Am Med Assoc 1997; 278:399-411.
106. Danzig R, Berkowsky PB. Why should we be concerned
about biological warfare? J Am Med Assoc 1997; 278:431-443.
107. World Health Organization. Health aspects of chemical
and biological weapons: Report of a WHO group of consultants. <None Specified>
Anonymous1970; 72-99.
108. Wells RM, Sosa-Estani S, Yadon ZE. An unusual hantavirus
outbreak in southern Argentina: person-to-person transmission. Emerg Infect
Dis 1997; 3:171-174.
109. Simon JD. Biological terrorism: Preparing to meet
the threat. J Am Med Assoc 1997; 278:428-430.
110. Zilinskas RA. Iraq's biological weapons: The past
as future? J Am Med Assoc 1997; 278:418-424.
111. Eitzen EM. Use of biological weapons. In: Sidell
FR, Takafuji ET, Franz DR, editors. Medical aspects of chemical and biological
warfare. Falls Church, VA: Office of The Surgeon General, Department of the
Army, United States of America, 1997:437-450.
112. Leskov S, Kogan V. Military bacteriological programs
in Russia and USA are strictly secretive and represent a terrible threat to
the world. Izvestiya 1993; p. 15 Moscow:
113. Birch D. Bubonic plague sample delivered to white
racist. Baltimore Sun 1995; p. A-4 Baltimore, MD:
114. Evans ME, Friedlander AM. Tularemia. In: Sidell
FR, Takafuji ET, Franz DR, editors. Medical aspects of chemical and biological
warfare. Falls Church, VA: Office of The Surgeon General, Department of the
Army, United States of America, 1997:503-512.
115. Evans ME, Gregory DW, Schaffner W, McGee ZA. Tularemia:
A 30-year experience with 88 cases. Medicine 1985; 64:251-269.
116. Foshay L. Tularemia: A summary of certain aspects
of the disease including methods for early diagnosis and the results of serum
treatment in 600 patients. Medicine 1940; 19:1-83.
117. Capps L, Vermund SH, Johnsen C. Smallpox and biological
warfare: The case for abandoning vaccination of military personnel. Am J Public
Health 1986; 76:1229-1231.
118. McClain DJ. Smallpox. In: Sidell FR, Takafuji ET,
Franz DR, editors. Medical aspects of chemical and biological warfare. Falls
Church, VA: Office of The Surgeon General, Department of the Army, United States
of America, 1997:539-559.
119. Khodakevich L, Szczeniowski M, Manbu-ma-Disu. The
role of squirrels in sustaining monkeypox virus transmission. Trop Geogr Med
1987; 39:115-122.120. Fine PEM, Jezek Z, Grab B, Dixon
J. The transmission potential of monkeypox virus in human populations. Int J
Epidemiol 1988; 17:643-650.
121. Ricketts TF. The diagnosis of smallpox. London:
Cassell, 1908.
122. Downie AW, St.Vincent L, Meikeljohn G. Studies on
the virus content of mouth washings in the acute phase of smallpox. Bull WHO
1961; 25:49-53.123. Mitra AC, Sarkar JK, Mukherjee MK.
Virus content of smallpox scabs. Bull WHO 1974; 51:106-107.
124. Downie AW, Fedson DS, St.Vincent L, Rao AR, Kempe
CH. Haemorrhagic smallpox. J Hyg 1969; 67:619-629.
125. Baxby D. Poxviruses. In: Parker MT, Collier LH,
editors. Topley and Wilson's principles of bacteriology, virology, and immunity.
8th ed. London: Arnold, 1990:559-571.126. Lane JM, Ruben
FL, Neff JM, Millar JD. Complications of smallpox vaccination, 1968: Results
of ten statewide surveys. J Infect Dis 1970; 122:307127.
Hanna W. Studies in small-pox and vaccination. Bristol, England: Wright, 1913.
128. Freed ER, Richard JD, Escobar MR. Vaccinia necrosum
and its relationship to impaired immunologic responsiveness. Am J Med 1972;
52:411-420.
129. Jahrling PB. Viral hemorrhagic fevers. In: Sidell
FR, Takafuji ET, Franz DR, editors. Medical aspects of chemical and biological
warfare. Falls Church, VA: Office of The Surgeon General, Department of the
Army, United States of America, 1997:591-602.
130. Jahrling PB, Geisbert TW, Dalgard DW. Preliminary
report: Isolation of Ebola virus from monkeys imported to the USA. Lancet 1990;
335:502-505.
131. McCormick JB, King IJ, Webb PA. Lassa fever: Effective
therapy with ribavirin. N Engl J Med 1986; 314:20-26.
132. Halstead SB. Antibody, macrophages, dengue virus
infection, shock, and hemorrhage: A pathogenetic cascade. Rev Infect Dis 1989;
11:S830-S839.
133. Enria DA, Fernandez NJ, Briggiler AM, Lewis SC,
Maiztegui JI. Importance of neutralizing antibodies in treatment of Argentine
haemorrhagic fever with immune plasma. Lancet 1984; 4:255-256.
134. Jahrling PB, Frame JD, Rhoderick J, Monson MH. Endemic
Lassa fever in Liberia, IV: Selection of optimally effective plasma for treatment
by passive immunization. Trans R Soc Trop Med Hyg 1985; 79:380-384.
135. Shepherd AJ, Swanepoel R, Leman PA. Antibody response
in Crimean-Congo hemorrhagic fever. Rev Infect Dis 1989; 11:S801-S806.
136. McKay DG, Margaretten W. Disseminated intravascular
coagulation in virus diseases. Arch Intern Med 1967; 120:129-152.
137. Cavanaugh DC, Cadigan FC, Williams JE, Marshall
JD. Plague. In: Ognibene AJ, Barrett ON, editors. General medicine and infectious
diseases. Washington, D.C. Office of The Surgeon General and Center of Military
History, 1982;
138. Brubaker RR. Factors promoting actue and chronic
diseases caused by Yersiniae. Clin Microbiol Rev 1991; 4:309-324.
139. Ehrenkranz NF, Meyer KF. Studies on immunization
against plague, VIII: Study of three immunizing preparations in protecting primates
against pneumonic plague. J Infect Dis 1955; 96:138-144.
140. Speck RS, Wolochow H. Studies on the experimental
epidemiology of respiratory infections, VIII: Experimental pneumonic plague
in Macacus rhesus. J Infect Dis 1957; 100:58-68.
141. Efficacy of killed whole-cell vaccine against a
lethal aerosol challenge of plague in rodents. Pitt MLM, Estep JE, Welkos SL,
Friedlander AM. Las Vegas: 1994;
142. Meyer KF, Cavanaugh DC, Bartelloni PJ, Marshall
JD, Jr. Plague immunization, I: Past and present trends. J Infect Dis 1974;
129(suppl):S13-S18.
143. Marshall JD, Quy DV, Gibson FL. Asymptomatic pharyngeal
plague infection in Vietnam. Am J Trop Med Hyg 1967; 16:175-177.


















