CUTANEOUS HUMAN PAPILLOMAVIRUS
INFECTIONS
Mark Naylor, M.D.
Disclaimer
Although available to the public via the Internet, this material is
targeted to an audience of trained clinical dermatologists.
Treatments and techniques described herein should only be done under
the supervision of a physician experienced in their proper
application. Failure to adhere to this guideline will substantially
increase the risk of serious adverse consequences, including bodily
injury or death.
Introduction
Introduction
Verruca (warts) are proliferative foci of epithelial keratinocytes
infected with human papillomaviruses (HPVs), DNA viruses which
replicate in epithelial cells. Because papillomaviruses are
specialized for replication in external epithelia, infections are
limited in scope to skin and mucosal surfaces exposed to the external
environment (HPV electron
micrograph).
Over 70 distinct human papillomavirus types are currently recognized.
Identification of new types is based on the degree of DNA
hybridization with previously classified types. If there is more than
a 10% difference from previously classified types, an isolate is
considered to represent a distinct type. Although there are many
exceptions, HPV types tend to cause characteristic clinical
lesions. Table 1 lists
the typical clinical lesions seen with HPV types.
Warts are usually spread by direct skin-to-skin inoculation of the
virus from one person to another, although transmission by fomites
also probably occurs. The mechanisms by which virions penetrate the
stratum corneum and infect viable keratinocytes is poorly understood.
The lack of a practical in vitro culture system for these
viruses has contributed substantially to the difficulty of studying
them.
The time between inoculation and the appearance of a lesion is quite
variable. Clinical experience suggests that it varies from one to a
few weeks for common warts to a year or more for some cases of
genital warts. The long latency of genital warts has caused confusion
with sexual abuse, since inoculation of infants from an infected
birth canal may not manifest in some cases for over a year.
Cell-mediated immune responses to the virus are probably the most
important factor in host
resistance [1-4].
Infiltrating T-cells and the satellite cell necrosis indicative of
cell-mediated keratinocyte death observed in regressing warts
supports this concept [5]. Obalek showed a
number of defects in cell mediated immunity in individuals with warts
including diminished dinitrochlorobenzene (DNCB) sensitivity in
patients with common and flat warts, and diminished peripheral blood
lymphocyte responses to phytohemagglutinin (PHA) in patients with all
types of warts [6].
Humoral immunity, on the other hand, does not appear to play a major
role in host responses or in treatment responses
[7]. 
Common Warts
Etiology
Common warts (verruca) are hyperkeratotic papulonodules most often
seen on the hands, arms and legs, but can be seen anywhere on the
glabrous skin (Figure
1a, Common Warts). Common verruca represent the most frequent
clinical lesions produced by the human papillomavirus. The morphology
can vary considerably from relatively smooth, sessile lesions as seen
in Figure 1b to large
pedunculated lesions as seen in Figure
1c. These are particularly common in childhood where immature
immunologic resistance and frequent skin-to-skin contact with peers
increases the likelihood of transmission. Another group who exhibit a
high infection rate are meat, poultry and fish
handlers [8, 9]. So
called "butchers warts" are usually caused by HPV 2 or 7
[10, 11]. The basis for the unusual
susceptibility of meat handlers has never been adequately explained
[11]. Individuals with atopic dermatitis
appear to have a mild T-cell defect as suggested by a higher
prevalence of infection and more numerous lesions. The presence of
atopy should be suspected when older children or adults present with
more than 10 common verruca and no other cause of
immunosuppression (Figure
2, Multiple Warts).
 Figure
1a. Common warts.
Figure
1a. Common warts.
A number of HPV types are known to cause what would be recognized
clinically as a common wart, including HPV 1, 2, 4, 7, 27, 57, 60, 65
[10]. HPV 2 is seen most frequently when
viral typing is done [12-14].
HPV types which cause common warts have a predilection for fully
keratinized epidermis and do not usually cause genital lesions
(condyloma acuminata). A notable exception is HPV 2 which is known to
cause common, oral and genital lesions and can cause autoinoculation
genital or oral warts from hand lesions [15-18].
The HPV 2 virus is a common cause of condyloma acuminata in young
children and infants. The virus can be spread from the hands of
infected caregivers during diaper changes, and therefore care should
be taken not to misconstrue autoinoculation or innocent contact
infections as evidence of sexual abuse.
Treatment
Treatment for warts can be divided into ablative and medical
approaches. Ablative methods include classic surgical excision and
destruction by electrodesiccation, laser or liquid nitrogen.
Intralesional bleomycin is an effective ablative treatment, although
unless this is used frequently and the cost shared among several
patients, the drug can be prohibitively expensive.
Vesicants such as cantharidin, alone or in combination with
podophyllin or other agents are an effective and almost painless
ablative therapy, making them a good choice for children. Caution
should be taken with these agents since the high surface area of
warts can lead to a more vigorous than expected response.
Liquid nitrogen is generally the ablative method of choice since it
can be rapidly applied to multiple lesions without local anesthesia
and is one of the least scarring approaches. Liquid nitrogen is a
good choice for cooperative adults with 1 to 6 glabrous skin lesions
not previously treated by other methods. Single lesion cure rates for
liquid nitrogen in experienced hands will generally be 80% for
appropriate lesion (less than 1 cm in diameter) in non-acral skin.
While surgical/ablative methods are less practical than medical
treatments for very large or numerous lesions, they have the
advantage of not requiring a high degree of patient compliance.
Medical therapies in experienced hands can be a much more effective
way to treat large or numerous warts. Drawbacks of these approaches
are that they requires more experience on the part of the clinician
and good patient compliance to achieve optimal results.
Topical medical therapy usually includes once or twice daily
application of cytotoxic or antiviral agents, including
5-fluorouracil, retinoic acid, podophyllin or podofilox. Keratolytic
agents such as salicylic acid/lactic acid combinations are useful,
particularly in combination with a cytotoxic agent. Treatment
duration will depend on the size of the wart and the degree of
discomfort tolerable to the patient, but generally will require 4-6
weeks or longer.
Topical immunotherapy, which involves the controlled induction of an
allergic contact reaction in the wart itself, can be done with
powerful haptens such as diphencyprone (DPC), squaric acid dibutyl
ester (SADBE) or dinitrochlorobenzene
(DNCB) [19] Topical
immunotherapy is one of the most potent ways to treat warts, and one
of the least scarring forms of therapy. These agents can be applied
by the physician, or in lower concentration, at home by the patient
[19]. These agents frequently cause
non-therapeutic allergic contact reactions, so good compliance with
instructions on the part of the patient, and caution and experience
on the part of the physician are necessary to achieve good results
with a minimum of side effects.
Systemic therapy with oral retinoids or H2 antagonists may be useful
for treating large numbers of warts. Isotretinoin or etretinate can
be used as monotherapy or as adjunctive therapy in combination with
topical therapy. H2 antagonists such as cimetidine and ranitidine
have been used to stimulate cell-mediated responses to the virus in
both children and adults [20-22].
While a recent controlled trial did not show a significant benefit of
cimetidine over placebo, H2 blockers may be efficacious in dosages of
30 mg/kg or greater (dosages from 25-40 mg/kg have been utilized in
most published studies), particularly as an adjunct to topical
therapy [23].
Young children have a high rate of so-called spontaneous resolution
of warts, the majority of which may be immunologic cures. Controlled
trials suggest that about 30% of children will respond to placebo
treatment within 3 months and more than 50% undergo remission without
treatment within two years [23-25]. These
facts have led to serious attempts to induce cures with suggestion
(sham treatment) using props such as UVA lights, fluorescent dyes or
other pseudo treatments. While this undoubtedly has the advantage of
not subjecting young children to painful and emotionally traumatic
treatments, the short term response rate can only be expected to be
approximately 30%, and it is therefore not preferable to more
effective and relatively painless therapies such as cantharidin and
topical 5-fluorouracil. Furthermore, untreated children are a
reservoir for the virus that can infect other children and adults,
perpetuating and intensifying the problem.
 Figure
3. Periungual Warts.
Figure
3. Periungual Warts.
Periungual warts require special therapeutic consideration (Figure
3, Periungual Warts). Selection of treatment will vary
considerable depending on the clinical situation. Although it has
been said that liquid nitrogen is the treatment of choice, this is
extremely uncomfortable and has the potential to permanently damage
the nail matrix. Bleomycin injections are also effective, but has
risks similar to liquid nitrogen (matrix damage) and very
occasionally can cause persistent Raynaud's phenomenon in treated
digits [26, 27].
Electrodesiccation under local anesthesia can be effective, but is
usually not the preferred initial method of treatment, since it is
one of the most scarring forms of therapy. Medical treatment with
combined topical therapies of various types is probably the least
scarring and most effective method of treatment, but requires good
patient compliance. 5-fluorouracil solution, retinoic acid solution,
and keratolytics containing salicylic acid, can be used as single
agents or for enhanced effectiveness, in combination. Topical
immunotherapy is an excellent form of therapy for resistant cases.
The preferred method of therapy will depend heavily on the clinical
situation and the experience of the treating physician. Further
treatment suggestions can be found in the RXDERM-L
Archive.
Palmo-Plantar Warts
These lesions are remarkable for their thickness due to their
presence in the acral skin of the hands and feet. The greater depth
of infected tissue makes these warts more difficult to treat
successfully compared with warts in non-acral skin.
Etiology
HPV 1 is the most common etiology of palmar and plantar warts,
although HPV 2 and other viruses cause
them [12, 28] (Figure
4a, 4b, 4c,
4d, Plantar
Warts; Figure
5, Palmar Wart). HPV 60, a much less common
cause of plantar warts, is associated with palmoplantar warts that
have cystic components. HPV 63, also an uncommon cause of plantar
warts, can cause a punctate mosaic-type plantar wart (Figure
4c).
 Figure
4b. Plantar wart
Figure
4b. Plantar wart
Treatment
Liquid nitrogen can be used, especially with small, early lesions.
Treatment of lesions larger than a centimeter in diameter with
nitrogen is frequently unsuccessful due to the pain involved in
freezing deeply enough to destroy all virus infected tissue.
Disadvantages of this approach are that a blister will almost always
be necessary to have a reasonable chance of cure with a single
treatment, and in some instances treatment may induce scarring (which
may be perceived by the patient as a persistence of the wart).
Incremental monthly, bimonthly or weekly liquid nitrogen followed by
paring of necrotic tissue can also be effective if done frequently.
In addition to liquid nitrogen, other forms of destructive treatment
can be used successfully including excisional surgery, and laser
ablation. Medical therapy is very effective, given good compliance
and a practitioner familiar with this form of therapy. An advantage
to medical treatment is that the activities of the patient are not
interrupted as they typically are in the healing phase of ablative
surgery. Daily or twice daily application of topical formalin, 10%,
in conjunction with aggressive paring of the wart has also been used
successfully. Topical treatments used in the treatment of other types
of warts can also be effective, including 5-FU 5%, topical retinoic
acid liquid 0.05%, and topical keratolytics. If available, topical
immunotherapy is probably the treatment of choice for large or
resistant lesions.
Verruca Plana (Flat
Warts)
 Figure
6a. Verruca plana.
Figure
6a. Verruca plana.
Etiology
Warts of this type are less exophytic than common warts,
frequently presenting as several or dozens of subtle papules 2-4 mm
in diameter elevated above the surface less than a millimeter or so
(See Figure 6a). These can be quite subtle,
and may be missed by a casual observer. Pigmentary disturbances may
be the most disturbing part of a flat wart infection to the patient
(See Figure
6b and 6c). These
lesions are frequently a problem on the face and glabrous skin of
non-immunocompromised individuals. Flat warts in this setting are
commonly caused by HPV 3, 10 and occasionally by HPV
2 [29-32]. A number
of other HPV types cause flat warts in glabrous skin (see
Table 1), but most of these are seen exclusively in
immunocompromised individuals and in epidermodysplasia verruciformis
(see Table 1) [33-35].
Treatment can be difficult even in an immunocompetent
individual.
Treatment
Medical therapy with a number of topicals can be tried, including
retinoic acid liquid (0.05%), topical 5-FU (either 2% or 5%),
podofilox, podophyllin or salicylic acid containing preparations
(Duofilm, Occlusal-HP, others). If monotherapy is not successful,
combinations of topicals agents can be tried. Ablative therapy,
particularly with liquid nitrogen is also useful. Topical
immunotherapy can also be used cautiously for difficult
cases.
Condyloma Acuminata
Etiology
Human papillomavirus types 6 and 11 are the most prevalent viral
types found in condyloma acuminata (Figure
7a, 7b, 7c, 7d)
[36-39]. Other virus types causing
mucocutaneous lesions in the genital region that are considered to be
at highest risk for causing cervical and cutaneous cancers include
HPV 16, 18 and several others (see Warts
& Cutaneous Carcinoma below).
 Figure
7b. Condyloma acuminata.
Figure
7b. Condyloma acuminata.
Treatment
Simple destruction with liquid nitrogen is effective in smaller,
well circumscribed lesions. Laser ablation is particularly good for
intravaginal or cervical lesions where simpler destructive techniques
(e.g. liquid nitrogen) are technically difficult to use.
Topical trichloroacetic acid has also been applied to ablate lesions.
Larger or more extensive lesions should probably be shrunk with
medical therapy prior to attempts at ablation.
A traditional treatment that is still very effective is application
of podophyllin 20-25%, in tincture of benzoin which generally
requires several treatments to be effective. This should be applied
by the physician, since over treatment may result in enough systemic
absorption to cause nervous system toxicity
[40].
Podofilox, one of the active ingredients in podophyllin is available
in the U.S. as Condylox, which can be applied by the patient. Topical
5-fluorouracil, 2%, is also effective and can be applied safely by
the patient. Patients should be cautioned not to overuse either of
these topical preparations, since extreme reactions may result. Even
when applied properly, a large wart with a correspondingly large
surface area may necrose rapidly under podophyllin treatment during
the initial stages of treatment, necessitating symptomatic
treatment.
Cytokines such as interferon alfa-2b, 1 million units delivered
intralesionally three times weekly for 3 weeks can be tried. Topical
immunotherapy can be used cautiously in resistant cases. Newer agents
such as cidofovir and imiquimod may soon add to the topical
armamentarium for treatment of condyloma.
Because viral typing is not widely available as a clinical test, it
is reasonable to assume that an infection is due to a viral type with
a high risk for the subsequent development of cancer (see Warts
& Cutaneous Carcinoma below). Since infection with a high
risk virus type is only one step in the carcinogenic process,
infection with a high risk virus does not by itself mean that a
cancer will develop. However, it does increase the risk, particularly
if condyloma are allowed to remain untreated for several
years.
A treatment philosophy which reflects this is to treat all clinically
evident lesions aggressively until resolved and to follow for the
development of new lesions for several months. Relapses should be
treated aggressively. Affected females and female sexual partners of
affected males should have a pap smear and appropriate follow-up to
monitor for the development of cervical dysplasia.
Oral Warts
 Figure
8. Oral warts.
Figure
8. Oral warts.
Etiology
While not often recognized clinically, oral warts (Figure
8) are a surprisingly common subclinical infection in
non-immunocompromised individuals [41].
At least 90% of oral squamous papillomas and condyloma acuminatum can
be shown by in situ hybridization to harbor type 6 or 11 sequences
[42, 43].
Treatment
Simple destruction with liquid nitrogen, laser, or
electrodesiccation under local anesthetic is probably the best
approach for a few lesions. If oral papillomavirus infection is
associated with an immunocompromised state, the prognosis may reflect
the severity of the underlying immune deficiency.
Focal Epithelial
Hyperplasia
 Figure
9. Focal epithelial hyperplasia.
Figure
9. Focal epithelial hyperplasia.
Etiology
Focal epithelial hyperplasia (FEH) or Heck's disease (Figure
9) is a discrete, yet disseminated viral infection of the oral
mucosa. HPV 32 is the most common cause of this entity, with HPV 13
being the next most common [44].
Other viruses, including HPV 11, are known to give rise to the
characteristic findings occasionally. This is not known to be a
precancerous condition. In some cases there may be a familial
predisposition.
Treatment
Liquid nitrogen or laser treatment can be tried, but the lesions
tends to be resistant to destructive therapy and may resolve without
treatment. Other forms of therapy including intralesional interferon,
oral H2 blockers, oral retinoids, or topical therapy with 5-FU singly
or in combination with topical tretinoin may be
useful.
Epidermodysplasia
Verruciformis
 Figure
10a. Epidermodysplasia verruciformis.
Figure
10a. Epidermodysplasia verruciformis.
Etiology
Epidermodysplasia Verruciformis (EDV, Figure
10a, 10b, 10c,
10d, 10e) is an
autosomal recessive disorder of cutaneous immunity which makes
affected individuals susceptible to a subset of warts not seen in
other individuals. The advent of transplant technology and the AIDS
epidemic has changed this, and now cases of clinical infection with
these viruses are seen in immunocompromised
individuals [33, 34]. The
immune defect in the familial disorder appears to be a very narrow
problem that only makes them susceptible to the characteristic wart
types seen in EDV. HPV types characteristic of the disorder include
HPV 3, 5, 8, 9, 10, 12, 14, 17, 20, 21, 23, 25, 28, 38, 47,
49.
Warts in EDV are typically flat, numerous and subtle, but may be
erythematous (Figure 10d). When the disease
begins to manifest in childhood, the warts sometimes give the
clinical appearance of tinea versicolor. The warts can involve almost
any area on the body, but tend to be more prominent on the
extremities, especially the arms (Figure
10a).
The fact that immune suppression from other causes also results in
susceptibility to this unique group of papillomaviruses is itself
indirect evidence for the central role of an immune defect in EDV
[33, 34]. Further evidence for a
dysfunction in cell mediated immunity comes from the observation that
60% of these individuals cannot be sensitized to DNCB [6].
Overproduction of tumor necrosis factor-alpha, transforming growth
factor-beta and cis-urocanic acid may be playing a role in the
familial immunologic defect [32].
The combination of HPV infection, relative immunosuppression and
sunlight are a potent carcinogenic combination; if these individuals
are not recognized and treated appropriately, they are at substantial
risk of developing skin cancer (Figure
10f--squamous cell carcinoma occuring in EDV
and Figure
10g--Bowen's disease on the ear in EDV).
Treatment
Destruction with liquid nitrogen or other ablative techniques can
be used, particularly to clear sun exposed areas at greatest risk for
malignant transformation. Medical therapies such as topical
retinoids, or 5-FU are useful for treating more widespread
involvement. Topical immunotherapy or one of the newer topicals such
as imiquimod or cidofovir should be considered. Oral retinoids or H2
blockers may be useful in combination with topical therapies. Sun
exposure is an important cofactor in the development of squamous
malignancies in these individuals, and sun protection measures should
be pursued vigorously. X-ray treatment of EDV associated squamous
neoplasms should be avoided, since it may stimulate malignant
degeneration in adjacent lesions and make recurrences more aggressive
[32].
Warts & Cutaneous
Carcinoma
The carcinogenic nature of certain subtypes of the human
papillomavirus has been recognized now for over a decade. While the
female genital tract, particularly the cervix, is most prone to the
carcinogenic effect of these viruses, glabrous skin can also be
involved.
The most carcinogenic of these viruses are types which cause genital
or oral lesions, particularly, HPV 16, 18, 31, 33, 39, 35, 51, 58,
72, and 73. The other major group of papillomaviruses associated with
cancer are those associated with epidermodysplasia verruciformis,
particularly types 4, 5, 8, 14 and 47. Tumors of the glabrous skin
generally involve the genital viruses, since the EDV-associated types
are rarely seen in non-immunocompromised individuals. Clinical
lesions can include verrucous and squamous cell carcinomas of the
genital regions or perineum and squamous carcinomas of the fingertips
and plantar skin. Condyloma acuminata of the perianal region
(Figure 7d) can also predispose to rectal
carcinoma, particularly when the condylomas are due to a high risk
virus.
Mechanisms of
Carcinogenesis
Cancer can be viewed as the accumulation of 3-5 heritable
abnormalities that work in concert to produce a fully malignant cell.
This is shown schematically in Figure 11. Infection with a human
papillomavirus, particularly a high risk virus, can account for at
least two potentially serious molecular defects, namely loss of p53
and/or retinoblastoma protein function.
Figure 11. Genetic events in carcinogenesis. The first genetic
change that predisposes to carcinogenesis has been termed initiation.
Accumulation of additional genetic abnormalities occurs during
progression until enough have accumulated to result in a fully
malignant cell type (generally, 3-5 genetic abnormalities). Clonal
expansion during this process results in a tumor.
Human papillomaviruses have evolved proteins to control the growth of
the epithelial cells they infect. This was a necessity since these
viruses require a metabolically active, dividing cell in order to
complete their life cycle. In particular, the E6 and E7 proteins have
the ability to abrogate growth and differentiation controls that
would otherwise prevent epithelial cell growth and stymie viral
propagation (see Figure 12). The "E" designation indicates an early
gene, meaning a viral gene that is turned on early in the process of
infecting a cell.
Figure 12. The human papillomavirus genome. The "E"
designation indicates an early viral protein which is expressed early
in a vegetative infection. Similarly, the "L" designation indicates a
late viral gene, usually involved in viral protein coats.
The E7 protein targets the retinoblastoma protein, a critical
component of cell cycle control. The retinoblastoma protein (Rb) in
the unphosphorylated state binds to and sequesters transcription
factors necessary for progression through the cell cycle,
particularly E2F and related proteins. This prevents cells from
dividing until E2F becomes available in the unbound state, usually by
release from Rb. In normal cellular physiology, this release is
accomplished by Rb phosphorylation by one of the cyclin-dependent
kinases. In the case of a papillomavirus infection, E2F release is
due to binding of Rb by viral E7 protein (see Figure
13).
Figure 13. E7 Effects on Rb. E7 binding of RB leads to release
of sequestered E2F, enabling the cell cycle to progress.
Rb is a classic example of a tumor suppressor gene. Tumor suppressor
genes are normal genes whose loss of function predisposes the cell to
cancer. These genes are involved in various important processes
critical to cellular homeostasis, including differentiation, DNA
repair, control of the cell cycle and apoptosis. Complete loss of
function of the retinoblastoma gene is seen in conjunction with a
number of tumors including retinoblastomas and melanomas. The
relative carcinogenic potency of the various human papillomavirus
types is partially explained by the relative avidity of their
respective E7 proteins for Rb, e.g., the more tightly a given
viral E7 binds Rb, the greater the oncogenic potential of the
virus [45].
The other important tumor suppressor gene involved in viral
carcinogenesis is p53, which has at least three important functions
involved in its tumor suppressor role (see Figure 14). In response to
DNA damage, p53 stops cell division and up-regulates genes involved
in DNA repair such as Gadd45 [46]. If the
DNA cannot be repaired, p53 performs its third and perhaps most
crucial function, to induce programmed cell death. This ensures that
no unrepaired DNA damage is propagated, and is vitally important to
maintaining the integrity of the genome. Because of these crucial
functions, p53 has been termed the "guardian of the genome".
Therefore, loss of p53 promotes genetic instability and strongly
predisposes affected cells to accumulate additional genetic
abnormalities.
Figure 14. Function of p53. The E6 viral protein binds to and
inactivates p53.
Because p53 is also important in regulating differentiation and
suppressing cell division, human papillomaviruses have evolved the E6
protein to circumvent it. Analogous to E7 proteins, E6 proteins of
the high risk viruses bind p53 with greater avidity. In addition, the
most oncogenic viruses actually promote ubiquitin-mediated p53
breakdown, leading to a profound loss of p53
activity [47].
Vegetative infections with human papillomavirus are generally
characterized by episomal replication of the viral genome. However,
in most HPV-associated tumors, integration of papillomavirus DNA into
chromosomal DNA is observed [48].
Integration may itself be involved in the tumorigenicity of
papillomaviruses. Integration is usually necessary for
immortalization of keratinocyte cell lines with papillomaviruses
[49, 50]. Not surprisingly, E6 and E7
sequences are the most common viral genes included in integrations
associated with tumors and appear to be the portion of the viral
genome essential for immortalizing keratinocyte lines [51].
Loss of expression control of the E6 and E7 genes may occur during
integration. This may be due in many instances to loss of the E2
gene, a common event during integration. The E2 protein product is
involved in regulating the expression of other viral genes, including
E6 and E7 [52, 53]. Expression of
integrated E6 and E7 genes could also be enhanced due to factors
associated with the host cell genome. In support of this concept, one
study noted that clonal cell populations with integrated E7 sequences
had higher levels of E7 expression compared with clones without
integration, in spite of a higher E7 copy number in non-integrated
clones [54].
Another mechanism which may be operative is the physical interruption
or disruption of function of important cellular tumor suppressor
genes caused by the random integration of viral sequences. This idea
is supported by the large number of integration sites seen in some
studies where this has been determined, consistent with a greater
chance of interrupting important cellular control genes
[54].
Bowen's
Disease
 Figure
15. Bowen's Disease in the natal cleft.
Figure
15. Bowen's Disease in the natal cleft.
Bowen's disease, particularly when found in the perineal region,
can be related to condyloma acuminata (Figure
15). In this case, there was a 15 to 20 year history of
preexisting, inadequately treated condyloma acuminata. A lesion which
still resembles a wart grossly and microscopically can be see in the
lower right portion of the image. The reddest area had a foci of
invasive squamous cell carcinoma when it was removed. Other Bowen's
tumors located in non-sun exposed areas may be related to
papillomavirus infection (Figure
16a-16b). Clinically and histologically,
these lesions have features of viral warts.
Bowenoid
Papulosis
 Figure
17b. Bowenoid papulosis on scrotum. 17c is a close-up of this
same lesion.
Figure
17b. Bowenoid papulosis on scrotum. 17c is a close-up of this
same lesion.
Bowenoid papulosis (Figure 17a, 17b,
17c) is a hyperkeratotic genital lesion that
is clinically compatible with a benign papular wart, yet has an
histology compatible with squamous cell carcinoma in situ
(Figure 17c). It has been said that these
are not likely to progress to an invasive lesion. However, since a
high percentage of these lesions harbor a high risk virus, the wisest
course is to destroy them.
Other
Malignancies Related to the Human Papillomavirus
Other malignancies related to human papillomaviruses include
verrucous and squamous cell carcinomas of the penis, plantar skin or
vulva, and squamous cell carcinomas of the periungual region of the
finger. Uncircumcised males have the greatest risk of developing
carcinoma of the penis because of the co-carcinogenic influence of
smegma (the mixture of cellular debris and toxic substances that
builds up under the foreskin). The finger is prone to these problems
because of its occasional contact with genital skin harboring high
risk viruses and the co-carcinogenic effect of
sunlight.
References
1. Rogozinski TT, Jablonska S,
Jarzabek-Chorzelska M: Role of cell-mediated immunity in spontaneous
regression of plane warts. Int J Dermatol 27(5):322-326, 1988.
Human papillomavirus-induced plane warts most often occur in the
second decade of age. Afterward, they either spontaneously regress or
are eradicated in the course of various treatments. As proved by in
vivo and in vitro tests as well as clinical observations, they most
often affect and persist longer in immunocompromised hosts. In this
work it was confirmed that specific-ie, anti-HPV-directed,
cell-mediated immunologic response plays a role in spontaneous
regression of plane warts and that preservation of nonspecific
immunity is prerequisite for spontaneous regression of plane
warts.
2. Avgerinou G, Georgala S, Theodoridis A, et al.: Reduction of
cell mediated immunity in patients with genital warts of long
duration. Genitourin Med 62(6):396-398, 1986. Cell mediated
immunity was studied by a leucocyte migration inhibition assay and by
tuberculin and dinitrochlorobenzene skin tests in 30 patients with
recurrent genital warts and in 34 healthy people (with no history of
genital warts) who served as controls. Migration inhibition was
significantly less in patients suffering from recurrences for more
than one year than in controls (p less than 0.001).
Dinitrochlorobenzene and tuberculin sensitivity were also found to be
impaired in those with infection of long duration (p less than
0.001).
3. Stanley M, Coleman N, Chambers M: The host response to lesions
induced by human papillomavirus. Ciba Found Symp 187:21-32;
discussion 32-44, 1994. Human papillomaviruses (HPVs) are
strictly intraepithelial pathogens: in the natural productive
infection they induce benign epithelial proliferations of
mucocutaneous surfaces, some of which may progress to malignancy.
Benign HPV-induced lesions are chronic persistent growths; high
levels of viral antigen are expressed in the apparent absence of a
host immune response suggesting that these viruses have evolved
efficient mechanisms of immune evasion. Cell-mediated responses are
central in the pathogenesis of HPV and regression of both cutaneous
and genital warts histologically resembles a delayed-type
hypersensitivity response (DTH). The antigen(s) in the wart against
which this response is initiated are not known but in an experimental
murine model DTH responses to the E6 and E7 proteins of HPV-16 can be
elicited when viral antigen is presented via the epithelial route.
Priming with low levels of viral antigen in this model induces
non-responsiveness and the loss of DTH. In HPV-associated cancers the
E6/E7 genes are expressed and an antibody response to the proteins is
found in at least 50% of cases indicating that these oncoproteins are
potential targets for immunotherapy. [References:
22]
4. van der Steen P, van de Kerkhof P, der
Kinderen D, et al.: Clinical and immunohistochemical responses of
plantar warts to topical immunotherapy with diphenylcyclopropenone. J
Dermatol 18(6):330-333, 1991. A 30-year-old man with bilateral
plantar warts of the mosaic type which had been resistant to standard
treatment modalities was treated with diphenylcyclopropenone. After
10 weeks, the treated warts had disappeared; the untreated warts,
although showing some involution, still persisted. The untreated
warts, serving as a control to prove the effectiveness of topical
immunotherapy, responded likewise to subsequent treatment with
diphenylcyclopropenone. Wart regression was reflected
histopathologically by decreases in acanthosis, papillomatosis,
granular vacuolation, and hyperkeratosis. Immunohistochemically,
Ki-67 expression was markedly reduced, and a reversal of the CD4/CD8
ratio was seen. These findings suggest a major role of a
cell-mediated immune response in the spontaneous resolution of
warts.
5. Iwatsuki K, Tagami H, Takigawa M, et al.:
Plane warts under spontaneous regression. Immunopathologic study on
cellular constituents leading to the inflammatory reaction. Arch
Dermatol 122(6):655-659, 1986. Immunohistologically, cellular
infiltrates in regressing plane warts were mainly composed of
lymphocytes and mononuclear phagocytes. There were many infiltrating
T lymphocytes. Immunoelectron microscopic observation demonstrated
that both helper/inducer and suppressor/cytotoxic phenotypes of T
lymphocytes infiltrated in the lesions. OKT6-positive cells were
observed in the dermis as well as in the epidermis. Moreover, as
noted in allergic contact dermatitis, the apposition of T lymphocytes
to Langerhans' cell-like cells could be seen. Lymphocytes and a small
number of mononuclear phagocytes were found adjacent to damaged
keratinocytes in the epidermis, the picture of which has been
described as satellite cell necrosis, a hallmark of cytotoxic
reaction by aggressors. These findings suggest that specific
cell-mediated immunity against virus-infected keratinocytes takes
place in the process of regressing plane warts.
6. Obalek S, Glinski W, Haftek M, et al.:
Comparative studies on cell-mediated immunity in patients with
different warts. Dermatologica 161(2):73-83, 1980. The
distribution of peripheral blood T and B lymphocytes, the in vitro
lymphocyte response to PHA, and in vivo experimental DNCB
sensitization were studied in patients with different clinical forms
of warts (common, 84; flat, 88; plantar, 22; genital, 14) and in 15
cases of epidermodysplasia verruciformis (EV). The percentage of T
lymphocytes forming E rosettes was significantly decreased in
patients with common (54.8%), flat (47.5%) and plantar (58.3%) warts,
and those with EV (47.6%) in comparison with normal controls (68.4%).
The DNCB sensitivity developed less frequently and it was less
intensive in patients with common and flat warts than in the normal
population. 60% of EV cases were anergic to challenging doses of
DNCB. The lymphocyte response to PHA was reduced in all groups of
patients studied as compared to normals. T cell function was found to
be most defective in patients with EV and those with flat warts. Only
a slight but statistically significant defect was demonstrated in the
common wart group. CMI in patients with both plantar and genital
warts was shown to be almost normal; except minor alterations of
PHA-induced lymphocyte transformation and E rosetting T lymphocyte
counts. These data have shown the divergency of CMI defect in the
patients with different clinical forms of warts caused by various HPV
types. This could indicate that distinct HPV types varied in their
infectiveness and host cell-mediated resistance is a fundamental
factor preventing viral infection.
7. Steele K, Shirodaria P, O'Hare M, et al.:
Monochloroacetic acid and 60% salicylic acid as a treatment for
simple plantar warts: effectiveness and mode of action. Br J Dermatol
118(4):537-543, 1988. Monochloroacetic acid crystals and 60%
salicylic acid ointment was found to be more effective than placebo
as a treatment for simple plantar warts in a double blind study on 57
patients. Nineteen (66%) patients in the active treatment group
compared with five (18%) patients in the placebo group were cured
after 6 weeks (P = 0.002). The active treatment was associated with a
significantly higher cure rate 6 months after entry (P = 0.04).
Treatments were well tolerated. IgG or IgM antibodies or both to
human papilloma virus (HPV) types 1 or 2 or both were detected
significantly more frequently in the actively treated group 6 weeks
after entry (P = 0.0005). Twelve (50%) patients considered to be
cured had no detectable secondary immune response. Our results
suggest that cure does not depend primarily on the humoral system but
rather on mechanical destruction of wart tissue, or occurs as a
result of cell mediated immunity.
8. Kilkenny M, Marks R: The descriptive
epidemiology of warts in the community. Australas J Dermatol
37(2):80-86, 1996. Warts are common skin infections caused by
human papillomavirus (HPV) and affect most people sometime in their
life. A number of epidemiological studies on the prevalence of warts
have been completed in schools, various occupational groups, general
practices and hospitals. All studies have relied on a subjective
measure for the diagnosis of warts. Cross-sectional studies completed
in schools have shown the prevalence in children to vary from 2 to
20%. Occupational handlers of meat, poultry and fish have a higher
prevalence than other workers. Children and young adults are the
groups most affected. Future studies are needed to investigate the
true frequency of warts in the community and the likelihood of an
individual developing these lesions during his/her lifetime.
[References: 40]
9. Rudlinger R, Bunney M, Grob R, et al.: Warts in fish handlers.
Br J Dermatol 120(3):375-381, 1989. Fish handlers frequently
suffer from hand warts. The clinical form and HPV type in these
lesions were studied. Eleven individuals (10 fishmongers and one
fisherman) with multiple hand warts were examined clinically and
samples from their warts examined by Southern blot and reverse blot
analysis. Clinically, with one exception, the warts were of the
common type. HPV DNA was detected in all but one individual. HPV4 was
found in one sample, HPV1 related virus in three, a virus hybridizing
with both HPV27 and HPV2 in five (four individuals) and HPV7 in seven
(six individuals). More than one type was detected in four
individuals. HPV7 infection was related to the greater length of time
spent in handling fish. These findings indicate that HPV7 is not, as
was previously thought, found exclusively in those handling butcher
meat and suggest that environmental conditions may be a factor in the
clinical manifestation of HPV7 infection. The exact nature of a virus
designated HPV2/27 and the significance of its presence in these fish
handlers remains uncertain.
10. Jackson V, Chalkley R: Separation of newly
synthesized nucleohistone by equilibrium centrifugation in cesium
chloride. Biochemistry 13(19):3952-3956, 1974.
11. Keefe M, al-Ghamdi A, Coggon D, et al.:
Cutaneous warts in butchers. Br J Dermatol 130(1):9-14, 1994.
Several studies have indicated a high prevalence of hand warts in
meat handlers, although the reasons for this are not clear. The high
prevalence may be partly due to HPV7, a virus found almost
exclusively in meat handlers, but the source of HPV7 is not known. We
have carried out a cross-sectional survey of hand warts in male meat
workers and controls from other occupational groups, to investigate
the reasons for the high prevalence of warts, and particularly of
HPV7, in butchers. We studied 240 abattoir workers, 246 retail and
wholesale butchers, 308 engineering fitters and 292 office workers.
Each subject was interviewed using a standard questionnaire, and his
hands were examined by a dermatologist. Scrapings from the warts were
tested for HPV1, HPV2 and HPV7 by a polymerase chain reaction method.
The prevalence of hand warts was 33.3% in the abattoir workers, 34.1%
in the butchers, 19.5% in the engineers and 14.7% in the office
workers. Scrapings were taken from 247 of 267 subjects with warts,
and HPV DNA was detected in 151 samples. The most common viruses were
HPV2 (94 men) and HPV7 (76 men). The excess of warts in meat workers
was largely due to HPV7, which was found in only two of the office
workers, and was not found in any of the engineers. Logistic
regression analysis showed no association between the prevalence of
hand warts (or HPV2 and HPV7 specifically) and hand trauma, cold and
wet working conditions, smoking, atopy, or handling any particular
kind of meat. We suggest that some constituent of animal flesh
predisposes to replication of HPV7 in keratinized
epithelium.
12. Corley E, Pueyo S, Goc B, et al.:
Papillomaviruses in human skin warts and their incidence in an
Argentine population. Diagn Microbiol Infect Dis 10(2):93-101,
1988. Human papillomavirus genomic types present in human warts
of an Argentine population were studied. HPV DNA from single warts
was obtained using an alkaline extraction procedure that resulted in
a clean DNA preparation, which could be analyzed with several
endonucleases. This method was used to isolate and insert the HPV
DNAs of two genomic types into the Bam HI site of the pBR322 plasmid.
Restriction maps of both HPV DNAs were constructed. According to
these maps, one of the genomic variations was identical to HPV1a and
the other to HPV2a. The incidence of HPV2 and of HPV1 in different
types of skin warts was studied by a dot blot hybridization assay.
Twenty-two out of 28 common warts were positive for HPV2 and negative
for HPV1; four were positive for HPV1 and negative for HPV2 and two
were negative for both. Five out of six plantar warts were positive
for HPV1, and one was negative for both. Three out of seven filiform
warts were positive for HPV2, three were positive for both probes,
and one was negative for both. Southern blot analysis of HPV2
positive samples indicated that 80% were HPV2a and 20% another
subtype not yet characterized. All plantar warts contained HPV1a. Msp
I/Hpa II restriction analysis confirms previous results indicating
that HPV1a DNA is partially methylated, while no evidence of
methylation was found for HPV2a DNA.
13. Rubben A, Krones R, Schwetschenau B, et al.:
Common warts from immunocompetent patients show the same distribution
of human papillomavirus types as common warts from immunocompromised
patients. Br J Dermatol 128(3):264-270, 1993. We studied the
papillomaviruses (HPV) found in 131 common warts from 111
immunocompetent patients by amplification of viral DNA sequences with
the general-primer-mediated polymerase chain reaction (PCR). The
virus types were determined by restriction-enzyme cleavage and
reverse-blot analysis. Results were confirmed by using the Southern
blot technique. Forty patients harboured HPV 2a, 25 individuals
showed HPV 2c and 13 yielded HPV 57. Common warts from 16 patients
were induced by a variant of HPV 57. HPV 7 was found in four
patients. HPV 1 was identified in two patients, and there was
evidence for HPV 4 in only one case. One individual yielded an HPV
type which was only weakly related to HPV 2. Three patients were
infected by more than one HPV type. PCR did not demonstrate HPV-DNA
in warts from six individuals. The distribution and variation of HPV
types found in the common warts of immunocompetent patients were
similar to the findings in immunocompromised patients reported by
other authors.
14. Nuovo GJ, Lastarria DA, Smith S, et al.: Human papillomavirus
segregation patterns in genital and nongenital warts in prepubertal
children and adults. Am J Clin Pathol 95(4):467-474, 1991. This
study compared the segregation patterns of human papillomavirus (HPV)
in genital and nongenital warts in prepubertal children and adults.
HPV 2 was detected in most nongenital warts in children and adults,
whereas neither HPV 6 or 11 was detected at nongenital sites in
either group with the use of in situ or Southern blot hybridization
analyses. Of nine genital tract lesions in children. HPV 2 was
detected in two and HPV 6 or 11 in six. More than 90% of cases of
regional tract condylomata in adults contained HPV 6 or 11. HPV 2 was
not detected in any of 99 genital tract lesions in adults. It is
concluded that HPV 6/11 cannot proliferate at nongenital cutaneous
sites and HPV 2 can proliferate in the genital tract of children but
not adults. Thus, the detection of HPV 6 or 11 in a genital wart in a
child implies, assuming cutaneous transmission, infection from a
genital site, whereas the detection of HPV 2 presumes nongenital
transmission.
15. Obalek S, Jablonska S, Favre M, et al.:
Condylomata acuminata in children: frequent association with human
papillomaviruses responsible for cutaneous warts. J Amer Acad
Dermatol 23:205-213, 1990.
16. Padayachee A: Human papillomavirus (HPV) types 2 and 57 in
oral verrucae demonstrated by in situ hybridization. J Oral Pathol
Med 23(9):413-417, 1994. Twenty-one cases of verrucae vulgaris
(oral warts) were investigated for human papillomavirus (HPV)-group
specific antigen by immunocytochemistry and for HPV types 1, 2, 4, 6,
11, 16, 18 and 57 by DNA in situ hybridization with biotinylated
probes. Twelve (57%) cases demonstrated the presence of HPV-group
specific antigen. Fifteen (71%) cases showed the presence of HPV DNA,
13 of which (87%) demonstrated both HPV types 2 and 57 in the same
cells and 2 of which (13%) demonstrated only HPV 2. Six cases were
negative for HPV 2 and 57 and all 21 cases (100%) were negative for
HPV types 1, 4, 6, 11, 16 and 18. Results indicate the association of
a new and as yet unidentified HPV type, closely related to HPV 2 and
57, with oral warts. The identification of both cutaneous type HPV 2
and another type closely related to HPV 2 and 57 in oral verrucae on
keratinized and non-keratinized mucosal surfaces indicates the
possibility of a latent infection; three patients had a history of
warts on their hands, suggesting autoinoculation. This study
indicated that future investigations of oral warts, based on a
correlation of clinical and histological features with HPV types by
DNA in situ hybridization, are called for.
17. Fierlbeck G, Rassner G, Pfister H: [Condylomata acuminata
in children--detection of HPV 6/11 and 2. Local therapy with
interferon-beta hydrogel]. Hautarzt 43(3):148-151, 1992. Four
cases of genital warts in children (girls) are reported. HPV 6/11-DNA
was identified in two cases, and HPV 2-DNA in one. In one case no
virus identification was possible. The clinical features of the HPV
2-induced genital warts showed the typical morphology of condylomata
acuminata. The mode of transmission of the virus, in absence of
sexual contact, could not be explained. The HPV 2-associated genital
warts might have been transmitted by autoinoculation from warts on
the hands. Topical treatment with IFN-beta-hydrogel was applied over
8 weeks, either as single-agent therapy (1 case) or as adjuvant
therapy after removal of the condylomata (3 cases). No remission was
seen with the single-agent therapy. In one case the genital warts
reappeared after adjuvant therapy, but in the other two cases no
recurrence was seen.
18. Obalek S, Misiewicz J, Jablonska S, et al.: Childhood
condyloma acuminatum: association with genital and cutaneous human
papillomaviruses [see comments]. Pediatr Dermatol
10(2):101-106, 1993. We studied 25 children, age 7 months to 12
years 6 months, with anogenital warts, and their parents. In most
children the warts were localized in the anal area, in 3 of 18 girls
perianally and on the vulva, and in 4 girls exclusively on the vulva.
Southern blot hybridization studies disclosed an association of
condylomata with human papillomaviruses (HPV) 6 and 11 in 74% and HPV
2 in 17.4% of patients. The clinical features were similar in warts
induced by genital and cutaneous HPVs. Even the HPV 2-associated
warts in the vulva of two girls were typical of condyloma acuminatum.
In all children with HPV 2-induced condylomata, cutaneous common
warts coexisted, also induced by HPV 2. However, three mothers had
cutaneous warts, and the children's condylomata were associated with
HPV 6. Thus, the mere presence of skin warts in family members does
not rule out other sources of infection. Sexual abuse was suspected
in four girls and two boys, but was not confirmed in any. Nonsexual
transmission could occur by persons with the lesions taking care of
children. Perinatal transmission also appears to be an important
route of infection in small babies. Infection in utero was probable
in one girl in whom anal warts appeared in the first week of life and
whose mother had cervical condylomata during pregnancy. This study
provides further confirmation of possible nonsexual transmission of
genital HPVs and the not infrequent association of childhood
condylomata with HPV 2.
19. Naylor M, Neldner K, Yarbrough G, et al.:
Contact immunotherapy of resistant warts. J Amer Acad Dermatol
19(4):679-683, 1988. Contact immunotherapy has been proved
effective in the treatment of resistant warts. This report chronicles
our experience with a new contact immunotherapy agent,
diphenylcyclopropenone. We have achieved a cure rate of 62% in 45
patients with resistant warts of all types who came to our general
dermatology clinic. Cure rates may be lower in patients who have
experienced multiple treatment failures. The majority of cures were
obtained within 3 to 4 months. Although it appears somewhat less
effective than published reports of dinitrochlorobenzene contact
immunotherapy, diphenylcyclopropenone contact immunotherapy is an
effective treatment for resistant warts and avoids any potential
problems from mutagenicity. [References: 31]
20. Glass AT, Solomon BA: Cimetidine therapy for
recalcitrant warts in adults. Arch Dermatol 132(6):680-682, 1996.
BACKGROUND: Common warts, or verrucae vulgaris, occur most often
in children. However, many adults are plagued by this ubiquitous
viral infection. Various modalities have been used to treat warts,
but none is uniformly effective or directly antiviral. A recent study
showed cimetidine to be effective in the treatment of multiple warts
in children. Anecdotal reports have suggested that the administration
of high doses of cimetidine, through various proposed
immunomodulating mechanisms, can improve recalcitrant warts in
adults. There have been no data published to date supporting these
claims. OBSERVATIONS: An open-label study was conducted to determine
the safety and efficacy of high-dose cimetidine in 20 adult patients
with recalcitrant warts. Of the 18 patients who completed the study,
16 patients (84%) had either dramatic clinical improvement or
complete resolution of their wart lesions after 3 months of
cimetidine therapy without any adverse effects. No patient
demonstrated disease progression while receiving the medication and
complete responders remained free of lesions at 1-year follow-up.
CONCLUSIONS: This study further confirms that high-dose cimetidine
therapy appears to be beneficial and safe in the treatment of
recalcitrant warts in adults. Further placebo-controlled studies are
needed to determine its true efficacy.
21. Bauman C, Francis JS, Vanderhooft S, et al.: Cimetidine
therapy for multiple viral warts in children. J Amer Acad Dermatol
35(2 Pt 1):271-272, 1996.
22. Orlow SJ, Paller A: Cimetidine therapy for multiple viral
warts in children. J Am Acad Dermatol 28(5 Pt 1):794-6,
1993.
23. Yilmaz E, Alpsoy E, Basaran E: Cimetidine
therapy for warts: a placebo-controlled, double-blind study. J Amer
Acad Dermatol 34(6):1005-1007, 1996. BACKGROUND: Cimetidine, an
H2-receptor antagonist, has been used successfully to treat patients
with mucocutaneous candidiasis, common variable immunodeficiency,
herpes simplex, and herpes zoster because of its immunomodulatory
effects. Recently, some trials have suggested that cimetidine may
also be useful for the treatment of warts. OBJECTIVE: The aim of the
present study was to determine whether cimetidine is effective in the
treatment of warts. METHODS: Seventy patients with multiple warts
were included in a placebo-controlled, double-blind study. Patients
were randomly allocated to treatment groups equally. The groups
received cimetidine, 25 to 40 mg/kg daily, or placebo for 3 months.
Patients were examined at monthly intervals. RESULTS: At the end of
the therapy, 28 cimetidine-treated and 26 placebo-treated patients
were examined to determine the efficacy of treatment. Cure rates
obtained were 32% (9 of 28) in the cimetidine-treated group and 30.7%
(8 of 26) in the placebo-treated group. No significant difference was
found between cimetidine and placebo in effectiveness (p = 0.85).
CONCLUSION: Our results show that cimetidine is no more effective
than placebo in the treatment of patients with common
warts.
24. Messing AM, Epstein WL: Natural history of warts: a two year
study. Arch Dermatol 87:301-310, 1963.
25. Esterly NB, Cutaneous viral infections, in Nelson's textbook
of pediatrics, R.E. Behrman and V.C. Vaughan, Editor. 1983, WB
Saunders: Philadelphia. p. 1721-1722.
26. Urbina Gonzalez F, Cristobal Gil MC, Aguilar
Martinez A, et al.: Cutaneous toxicity of intralesional bleomycin
administration in the treatment of periungual warts. Arch Dermatol
122(9):974-975, 1986.
27. Epstein E: Intralesional bleomycin and Raynaud's phenomenon. J
Amer Acad Dermatol 24(5 Pt 1):785-786, 1991.
28. Jenson AB, Lim LY, Singer E: Comparison of
human papillomavirus type 1 serotyping by monoclonal antibodies with
genotyping by in situ hybridization of plantar warts. J Cutan Pathol
16(2):54-59, 1989. Thirty plantar warts were analyzed for the
presence of HPV-1 type-specific and PV genus-specific capsid antigens
by immunofluorescence (IF) using monoclonal and polyclonal antibodies
and type-specific HPV-1 DNA employing in situ hybridization methods.
Fifteen of 30 plantar warts were positive by IF for PV genus-specific
structural viral antigens. Thirteen of the 15 productively infected
plantar warts expressed intranuclear HPV-1 type-specific capsid
antigens and viral DNA, which were detected in the same distribution
in each individual wart. The 2 productively infected plantar warts
that did not react with HPV-1 type-specific MoAbs did not react with
HPV-1 type-specific DNA by in situ hybridization. Thus, serotyping of
HPV-1 capsid antigens by monoclonal antibodies is concordant with
genotyping of HPV-1 viral DNA by in situ hybridization in
productively infected plantar warts.
29. Fuchs PG, Pfister H: Cloning and
characterization of papillomavirus type 2c DNA. Intervirology
22(3):177-180, 1984. Human papillomavirus (HPV) DNA was isolated
from a clinically diagnosed flat wart and proved to be related to
HPV2. The isolate showed 55% cross-hybridization with HPV2a. A
physical map of restriction enzyme cleavage sites differed completely
from those of HPV2a and HPV2b. The new HPV2 subtype, which will be
classified as HPV2c, was found to be very prevalent in common
warts.
30. Jablonska S, Orth G, Jarzabek-Chorzelska M, et al.:
Immunological studies in epidermodysplasia verruciformis. Bull Cancer
(Paris) 65(2):183-190, 1978. Immunofluorescence and cell mediated
immunity studies have been performed in 14 cases of epidermodysplasia
verruciformis (EV), 3 of those abortive or regressing in members of
the families of the patients with EV. Two different types of human
papillomavirus (HPV)--HPV3 and HPV4--have been found in cases of EV.
HPV3 was detected also in flat warts without features of EV. There
was no cross-reactivity between these two viruses, neither with HPV1
responsible for plantar warts nor with HPV2 inducing common warts.
There was a relationship between the type of HPV and the clinical
picture of EV as well as the malignant transformation, namely HPV4
has been found to be more oncogenic. Cell mediated immunity (CMI)
seems to be an important factor because it was depressed in a vast
majority of active cases and preserved in regressing and abortive
cases (in the members of the families of EV patients). However, low
CMI has been found in EV cases infected with HPV3 and in persistent
flat warts also due to HPV3, which did not undergo malignant
transformation. In contrast, in a case of EV due to HPV4 a malignant
transformation occured in spite of still preserved, although lowered
CMI. Various human papillomaviruses seem to differ in their oncogenic
potential. HPV1 responsible for plantar warts, and HPV2 for common
warts have no evident oncogenic potential, HPV3 inducing both EV and
flat warts has a low oncogenicity, whereas HPV4 inducing some cases
of EV seems more oncogenic.
31. Jablonska S, Orth G, Jarzabek-Chorzelska M, et al.: [New
developments relating to papillomaviruses]. Hautarzt 30(8):411-7,
1979. Molecular hybridization technique and immunofluorescence
studies with use of specific immune sera against the purified virions
isolated from various types of warts and wart-like lesions of
epidermodysplasia verruciformis (EV) made it possible to detect four
different types of human papilloma viruses (HPV). The recognition of
the viruses is important because of the different morphology of the
lesions induced and their various oncogenic potentials. HPV1 is
mainly responsible for plantar warts, HPV2 for common (hand) warts,
HPV3 has been found both in flat warts and in the variety of EV in
which skin lesions are of flat wart type, the course is relatively
more benign, and usually malignant transformation is not to be
expected. HPV4 was up to now found exclusively in the cases of EV
with prevalent red and red-brownish plaques and hyper- and
depigmentations similar to those of pityriasis versicolor. In all
cases of this variety of EV malignancies occured invariably. In
patients with EV, as also in--to a lesser extent--longstanding flat
and/or common warts cell mediated immunity was in general lowered,
but humoral specific anti-HPV antibodies were usually present. HPV
type seems to be of a decisive significance for potential
oncogenesis, because in a vast majority of cases EV due to HPV3 no
malignancies occured in spite of anergy, whereas malignant
transformation has been found in all cases due to HPV4, even in a
patient with still preserved, although lowered, CMI. [References:
47]
32. Majewski S, Jablonska S: Epidermodysplasia
verruciformis as a model of human papillomavirus-induced genetic
cancer of the skin. Arch Dermatol 131(11):1312-1318, 1995.
BACKGROUND: Epidermodysplasia verruciformis is a rare lifelong
disease that has raised an enormous interest since it is a model of
cutaneous genetic cancer induced by specific human papillomaviruses.
OBSERVATIONS: The interacting immunogenetic and environmental
factors, especially UV irradiation, result in the inability of the
patients' immune system to respond to epidermodysplasia
verruciformis-specific human papillomaviruses. The local
immunosuppression is an effect, at least in part, of the
overproduction of tumor necrosis factor alpha and transforming growth
factor beta1 and of the excessive formation of cis-urocanic acid.
CONCLUSIONS: Epidermodysplasia verruciformis is a model not only of
cutaneous viral oncogenesis but also of local defense mechanisms in
the progression of human papillomavirus-associated cancers.
[References: 62]
33. de Jong-Tieben LM, Berkhout RJ, Smits HL, et
al.: High frequency of detection of epidermodysplasia
verruciformis-associated human papillomavirus DNA in biopsies from
malignant and premalignant skin lesions from renal transplant
recipients. J Invest Dermatol 105(3):367-371, 1995. Based on
immunologic and epidemiologic data, it is plausible that skin cancer
in renal transplant recipients is associated with human
papillomaviruses (HPV). At present, conflicting evidence exists
concerning the presence of HPV DNA in these cancers. We recently
described a nested polymerase chain reaction method that enables the
detection of all previously isolated epidermodysplasia verruciformis
(EV)-associated HPVs. We now describe the detection of EV-associated
HPV DNA in 49 (80%) of 61 biopsies from squamous cell carcinomas, in
four (50%) of eight basal cell carcinomas, in 14 (93%) of 15 actinic
keratoses, in two (40%) of five cases of Bowen's disease, and in four
(57%) of seven keratoacanthomas. HPV DNA typing revealed that all
detected HPV types belonged to the EV-associated HPV types. A wide
spectrum of EV-associated HPVs was found, including six putative new
HPV types. In a high percentage of the lesions more than one HPV type
was detected. We often found the same HPV types in different skin
biopsies from both malignant and premalignant lesions from the same
patient. The high frequency of detection of EV-associated HPV types
in biopsies from malignant and premalignant lesions is in agreement
with the hypothesis that EV-associated HPVs are involved in the
pathogenesis of skin cancer in renal transplant
recipients.
34. Tieben LM, Berkhout RJ, Smits HL, et al.: Detection of
epidermodysplasia verruciformis-like human papillomavirus types in
malignant and premalignant skin lesions of renal transplant
recipients. Br J Dermatol 131(2):226-230, 1994. To evaluate the
putative role of human papillomaviruses (HPV) in the development of
skin cancer in renal transplant recipients, a series of skin biopsies
from premalignant and malignant skin lesions was analysed using the
polymerase chain reaction. Four different consensus primer pairs were
used. HPV DNA was detected in five of 24 cases of squamous cell
carcinoma, in one of three cases of Bowen's disease, in none of four
basal cell carcinomas, in two of seven cases of actinic keratosis and
in one of five cases of keratoacanthoma. Typing by direct sequencing
of the amplified HPV DNA was possible in seven of nine cases, and
revealed epidermodysplasia verruciformis (EV)-associated HPV types,
or HPV types related to EV-associated types. Hence, HPV DNA could be
detected in a significant proportion of (pre)malignant skin tumours
in renal transplant recipients. The finding that some of the detected
HPV types were as yet uncharacterized EV-related types, suggests that
HPV DNA could be present in a higher percentage of lesions, and might
be detected with refinement of the techniques.
35. Rudlinger R, Smith IW, Bunney MH, et al.: Human papillomavirus
infections in a group of renal transplant recipients. Br J Dermatol
115(6):681-692, 1986. One hundred and twenty renal transplant
recipients were investigated. Fifty-eight (48%) were found to have
warts, 13 (11%) keratoses and six (5%) to have, or recently to have
had cancers. The longer the time of immunosuppression, the greater
the prevalence of warts; of those patients who had had their
transplant for at least 5 years, 87% had warts. Those with a graft
survival time of 10 years or more are at special risk of warts,
keratoses and malignancy. Five (10%) of 50 women had genital warts,
four of whom had internal lesions (vaginal, cervical or anal) and one
developed a carcinoma of the vulva. These findings indicate the
advisability of colposcopy for all female renal transplant
recipients, a high risk group. Eighty-eight specimens from 42
patients were examined by DNA restriction enzyme analysis and cross
hybridization for the presence and type of human papillomavirus
(HPV). HPV DNA was detected in 66% of the warts examined, HPV2 and
HPV4 occurring most often and HPV1 and HPV3 only infrequently. In
sequential specimens from common hand warts of one individual, an HPV
was found which could not be precisely identified but was related to
HPV4. HPV16 was detected in a vaginal wart from one patient and an
HPV6-related virus in a vulval wart of another. HPV DNA of an unknown
type was demonstrated in one of 11 keratoses examined. With the
probes used to examine the few samples of skin cancers available,
HPV16 was found in a squamous cell carcinoma of the vulva, and faint
bands from an unidentified type of HPV were detected in two squamous
cell carcinomata from a patient's hand. One woman had plaque lesions
morphologically and histologically resembling those found in
epidermodysplasia verruciformis (EV). HPV5 was identified in these
lesions. This is only the third reported case of HPV5, previously
thought to be unique to EV, in a renal transplant
recipient.
36. Handley JM, Maw RD, Lawther H, et al.: Human
papillomavirus DNA detection in primary anogenital warts and cervical
low-grade intraepithelial neoplasias in adults by in situ
hybridization. Sex Transm Dis 19(4):225-229, 1992. In this study,
58 consecutive patients with primary anogenital warts were selected
from patients attending a genitourinary clinic. Patients were grouped
on the basis of clinical lesion site, i.e. patients with genital
warts only, patients with perianal or anal canal warts only, and
patients with concurrent perianal and genital warts. Of these
patients, 38% of the men (12/31) and 33.3% of the women (9/27) had
other anogenital infections, such as nonspecific urethritis (NSU) or
nonspecific genital infection, which were the most common. Of the
patients who had perianal warts, 37% of the men (7/19) and 25% of the
women (4/16) also had warts in the anal canal. Of the women who had
anogenital warts, 63% (17/27) had concurrent subclinical low-grade
cervical intraepithelial neoplasia (CIN) lesions. Human papilloma
virus (HPV) DNA (either 6 or 11, 16 or 18, or 31 or 33 or 35) was
detected in 53.3% (40/75) of the anogenital wart biopsy samples, and
in 35.2% (6/17) of the low-grade CIN lesions. HPV types 6 or 11 were
the most common types in anogenital warts (45.3%); and in CIN lesions
HPV types 6 or 11 and 16 or 18 were found with equal frequency (17.6%
each). There were no significant differences in HPV types between
patients with genital warts and patients with perianal and anal canal
warts. Anogenital infection with HPV is multicentric; external
anogenital warts and subclinical CIN lesions often exist
concurrently. The low prevalence of HPV DNA detected in anogenital
warts and CIN biopsy samples may be due to insensitivity of the in
situ hybridization technique used in this study.
37. Tsao YP, Yang KY, Han CP, et al.: Genital human papillomavirus
infections in Taiwan. International Journal of Gynaecology &
Obstetrics 44(1):39-45, 1994. OBJECTIVES: Identification and
typing of HPV infections in genital condyloma and normal cytological
cervix. METHODS: Cervical cells from 289 Pap cases with normal
cytological findings were examined for HPV infection by slot blot
hybridization. Fifteen condyloma biopsy specimens were studied by
Southern blot hybridization. RESULTS: Thirty-six cases (12.5%) with
normal cervical cytology were HPV positive. The predominant HPV type
in women with normal cytology is HPV-16. Risk factors for HPV
infection in women with normal cytology depend on age and history of
pregnancies. Twelve cases (80%) of condyloma contained HPV-6 or -11
sequences. The predominant HPV type in genital condyloma is HPV-11.
CONCLUSIONS: HPV detection in population-based screening programs for
cervical neoplasia can be an important tool in identifying women who
are at risk of developing dysplasia and cervical
cancer.
38. Czegledy J, Veress G, Konya J, et al.: Genital human
papillomavirus (HPV) infection in Hungarian women. Acta
Microbiologica Hungarica 40(2):115-122, 1993. The prevalence of
genital human papillomavirus (HPV) infection in Hungarian female
populations is not essentially different from that found in other
countries of Europe and North-America. Using filter in situ
hybridization (FISH), we found that, in a group of cytologically
normal women some low risk HPV types (such as HPV 6 and 11) and the
most important high risk HPV types (HPV 16 and 18) were present in
23% and 8%, respectively. Eighty-eight percent of condyloma
acuminatum patients harboured HPV 6 or HPV 11 in their tumours. On
the other hand, in precancerous lesions (cervical intraepithelial
neoplasia, CIN) HPV 16 was the predominant type, being present in
29-48% of patients, depending on the detection method used (Southern
blot hybridization vs. polymerase chain reaction). The detection rate
of high risk HPV types was found to rise with the increasing severity
of cervical neoplasia. Finally, 48% of invasive cervical carcinoma
specimens were positive for HPV 16 DNA in a type-specific polymerase
chain reaction. For patients with HPV 16 positive primary tumours,
all but one lymph node metastases and about 30% of histologically
normal lymph nodes proved positive for HPV 16 DNA. Our results--in
accordance with the numerous data found in literature--seem to
confirm the hypothesis that certain HPV types are greatly involved in
the development of cervical cancer.
39. Matsukura T, Sugase M: Identification of genital human
papillomaviruses in cervical biopsy specimens: segregation of
specific virus types in specific clinicopathologic lesions. Int J
Cancer 61(1):13-22, 1995. We have established a critical
identification method for the full spectrum of genital human
papillomaviruses (HPVs) in clinical specimens. It was based on the
recognition of PstI, BanI and MspI cleavage patterns of HPV DNA
detected by blot hybridization with HPV 58 DNA probe at Tm -40
degrees C. By this method, we identified 24 different types of
genital HPV including 5 novel types (HPV 59, 61, 62, 64 and 67) in
the specimens collected at one hospital and found almost all the HPVs
with the authentic cleavage patterns of their respective prototypes.
In 235 cervical biopsy specimens, HPV 6 or 11 was found in exophytic
condyloma acuminatum (15/15) but not in any cervical intraepithelial
neoplasia (CIN) specimens. In contrast, HPV 18, 30, 43, 54, 56, 59,
62, 66 and 67 were identified in CIN I (28/71) or II (4/56) but not
in CIN III, while HPV 16, 31, 33, 35, 39, 51, 52 and 58 were
identified in CIN III (83/93) as well as in CIN I (34/71) and II
(47/56). The result indicates that heterogeneous genital HPVs prevail
all over the world. In addition, HPV 6 and 11 are etiologic agents
only of exophytic condyloma, whereas the other HPVs are etiologic
agents of CIN with the segregation of specific HPVs in CIN III. We
propose a new clinicopathologic grouping of genital HPVs founded on
nucleotide homology of the HPV genome.
40. Fisher AA: Severe systemic and local
reactions to topical podophyllum resin. Cutis 28(3):233, 236, 242
passim, 1981.
41. Kellokoski JK, Syrjanen SM, Chang F, et al.:
Southern blot hybridization and PCR in detection of oral human
papillomavirus (HPV) infections in women with genital HPV infections.
J Oral Pathol Med 21(10):459-464, 1992. The presence of human
papillomavirus (HPV) in biopsies taken from clinically normal buccal
mucosa (n = 212) and clinical lesions (n = 60) was examined by
Southern blot hybridization (SBH) using 32P-labelled HPV DNA probes.
Furthermore, one hundred formalin-fixed, paraffin-embedded biopsies
were analyzed by using polymerase chain reaction (PCR), combined with
dot blot hybridization and biotinylated HPV DNA probes. With SBH and
PCR, 15.4% and 29.4% of the biopsies, respectively, contained HPV
DNA. In clinically normal epithelium, 15.6% and 23.1% of the samples
were HPV-positive with SBH and PCR, respectively. The HPV types
detected in the genital and oral mucosa of index patients differed in
all except two cases. Histology could not be relied on distinguishing
HPV DNA positive and HPV DNA negative samples. Hand warts were
encountered significantly more frequently in patients with a
concomitant oral HPV infection. To conclude, oral HPV infections as
detected by SBH and PCR are surprisingly common, but similar to the
genital tract, the virus seems to exist in a latent form in the vast
majority of cases. The frequent concomitant finding of skin warts and
oral HPV infection may suggest some kind of HPV-specific
immunosuppression.
42. Neville BW, Damm DD, Allen CM, et al., ed.
Oral & Maxillofacial Pathology. 1st ed. 1995, W.B. Saunders:
Philadelphia.
43. Miller CS, White DK, Royse DD: In situ hybridization analysis
of human papillomavirus in orofacial lesions using a consensus
biotinylated probe. American Journal of Dermatopathology
15(3):256-259, 1993. The effectiveness of the Viratype Omniprobe
in situ human papillomavirus tissue hybridization kit (Digene
Diagnostics) was evaluated for the detection of HPV DNA in common
orofacial lesions. Seventy mucocutaneous lesions were hybridized with
a biotinylated Omniprobe that was specific for HPV types 6, 11, 16,
18, 31, 33, 35, 42, 43, 44, 45, 51, 52, and 56. Eighteen (25.7%) of
the specimens analyzed had intranuclear positive signals for HPV.
Probing with HPV 6/11, 16/18, and 31/33/35 to delimit the HPV
genotype yielded HPV DNA 6/11 in 16 (88.9%) of the Omniprobe-positive
specimens. Only squamous papilloma and condyloma acuminatum were
found to harbor HPV DNA. Sites most frequently infected were the
labial and buccal mucosa (21.7%) and the floor of the mouth (17.4%).
These results suggest that hybridization with the Omniprobe provides
appropriate sensitivity and specificity for detecting HPV in some
benign proliferations of the oral cavity. However, the detection of
HPV in oral squamous cell carcinoma, lichen planus, and
keratoacanthoma remains problematic until more sensitive and specific
molecular techniques are used.
44. Padayachee A, van Wyk CW: Human
papillomavirus (HPV) DNA in focal epithelial hyperplasia by in situ
hybridization. J Oral Pathol Med 20(5):210-214, 1991. Eighteen
cases of focal epithelial hyperplasia (FEH) were investigated for the
presence of human papillomavirus (HPV) group specific antigen by
immunocytochemistry and HPV types 1, 6, 11, 13, 16, 18 and 32 by DNA
in situ hybridization employing biotinylated probes. Seven (39%)
specimens demonstrated the presence of HPV group specific antigen.
Fifteen (83%) specimens were positive for HPV DNA: 9 (60%) showed HPV
32, of which 6 were on non-keratinized mucosa and 3 on border of
keratinized and non-keratinized mucosa; 5 (33%) showed HPV 13, 4
lesions on keratinized mucosa and 1 on non-keratinized mucosa; 1 (7%)
specimen on non-keratinized mucosa showed HPV-11 related. Two
specimens on different sites from one patient showed the same HPV
type and one patient had, in addition to FEH, a squamous papilloma
also demonstrating the same HPV type. Results show a specific HPV
distribution pattern in the epithelium indicating areas of high viral
concentration adjacent to areas of low or no viral concentration.
This study also indicates the possibility of tissue-site specificity
or a latent infection and the possibility of a yet unidentified HPV
type associated with FEH. It is suggested that future monitoring of
patients be carried out with special reference to HPV type and
anatomical distribution pattern for FEH lesions.
45. Munger K, Yee CL, Phelps WC, et al.:
Biochemical and biological differences between E7 oncoproteins of the
high- and low-risk human papillomavirus types are determined by
amino-terminal sequences. J Virol 65(7):3943-8, 1991. Differences
in the biological characteristics of the high-risk human
papillomavirus type 16 (HPV-16) and the low-risk HPV-6 E7 proteins
were analyzed and shown to correlate with certain biochemical
properties. To ascertain which region of E7 conferred these
properties, chimeric E7 genes were constructed by the exchange of the
amino and carboxyl coding halves of the HPV-6 and HPV-16 E7 genes.
The amino-terminal half of E7 determined the affinity for binding to
the retinoblastoma protein pRB, the transformation properties, and
the ability to abrogate transforming growth factor beta-mediated
repression of the c-myc promoter. This region of E7 is therefore
responsible for the biological and biochemical differences between
the E7 proteins of the low-risk and the high-risk HPVs and
consequently is one of the critical determinants distinguishing these
two groups of viruses. Transcriptional transactivation of the
adenovirus E2 promoter, in contrast, was a property shared by E7
proteins of both low-risk and high-risk HPVs.
Author-abstract
46. Sanchez Y, Elledge SJ: Stopped for repairs.
Bioessays 17(6):545-548, 1995. The tumor suppressor protein p53
is intimately involved in the cellular response to DNA damage,
controlling cell cycle arrest, apoptosis and the transcriptional
induction of DNA damage inducible genes. A transcriptional target of
p53, Gadd45, was recently found to bind to PCNA, a component of DNA
replication/repair complexes, thereby implicating Gadd45 in DNA
metabolism. Using biochemical assays, a role for Gadd45 in excision
repair in vitro has been demonstrated. Antisense experiments have
also indicated an in vivo role for the GADD45 gene in UV-irradiation
survival. These discoveries establish a link between p53 and DNA
repair through Gadd45. [References: 27]
47. Scheffner M, Werness BA, Huibregtse JM, et
al.: The E6 oncoprotein encoded by human papillomavirus types 16 and
18 promoted the degradation of p53. Cell 63:1129-1136, 1990. The
E6 protein encoded by the oncogenic human papillomavirus types 16 and
18 is one of two viral products expressed in HPV-associated cancers.
E6 is an oncoprotein which cooperates with E7 to immortalize primary
human keratinocytes. Insight into the mechanism by which E6 functions
in oncogenesis is provided by the observation that the E6 protein
encoded by HPV-16 and HPV-18 can complex the wild-type p53 protein in
vitro. Wild-type p53 gene has tumor suppressor properties, and is a
target for several of the oncoproteins encoded by DNA tumor viruses.
In this study we demonstrate that the E6 proteins of the oncogenic
HPVs that bind p53 stimulate the degradation of p53. The E6-promoted
degradation of p53 is ATP dependent and involves the
ubiquitin-dependent protease system. Selective degradation of
cellular proteins such as p53 with negative regulatory functions
provides a novel mechanism of action for dominant-acting
oncoproteins.
48. Das BC, Sharma JK, Gopalkrishna V, et al.: A
high frequency of human papillomavirus DNA sequences in cervical
carcinomas of Indian women as revealed by Southern blot hybridization
and polymerase chain reaction. J Med Virol 36(4):239-245, 1992.
Ninety-six colposcopically directed biopsies from squamous epithelial
carcinoma of the uterine cervix and 22 age-matched normal control
biopsy specimens were examined by both Southern blot hybridization
and polymerase chain reaction (PCR) for the presence of different
human papillomavirus (HPV) DNA types. Cancer of the uterine cervix,
which is the most common malignant disease in Indian women, showed a
high frequency (98%) of HPV as compared to those reported from other
parts of the world. HPV type 16 was found to be the dominant (64%)
type while the frequency of HPV type 18 was very low (3%). On
individual typing of HPV, no biopsy was found to contain any other
known HPV types under stringent conditions of hybridization except a
single case of HPV type 11. Only one case of double infection with
HPV types 16 and 18 was recorded. Under low stringency conditions of
hybridization with a mixed probe of HPV types 16 and 18, 29
additional biopsies were found to be positive. Southern blot
hybridization alone detected HPV DNA in 92% of the cases but none in
the controls. By PCR, six (6.25%) more cases and four (18.18%)
healthy women were found to be positive for HPVs. Analysis of the
physical state of HPV 16 indicated integration in about 70% of
carcinoma cases while 30% of them were in episomal form. The findings
suggest that infection with HPV is an important etiologic factor for
the development of cervical cancer, that a number of such tumours may
arise without HPV infection, and that integration of the viral DNA
into host genome is not always essential for malignant
progression.(ABSTRACT TRUNCATED AT 250 WORDS).
Author-abstract.
49. Pirisi L, Creek KE, Doniger J, et al.:
Continuous cell lines with altered growth and differentiation
properties originate after transfection of human keratinocytes with
human papillomavirus type 16 DNA. Carcinogenesis 9(9):1573-1579,
1988. Immortalization of human keratinocytes (HKc) by human
papillomavirus type 16 (HPV16) is reproducible at a high frequency,
is due directly to the presence of the viral sequences in the cells,
and occurs independently from the genetic characteristics of the host
cells. Ten human keratinocyte strains, each derived from a different
individual, were transfected with pMHPV16d and selected with G418.
Eight became established lines. Two strains, which failed to grow
shortly after successful G418 selection, were negative for HPV16 DNA.
No lines were established following transfection of the same HKc
strains with vector sequences only. The immortalized lines maintained
a constant number of copies of the viral genome integrated into the
cellular DNA. Each line showed a unique integration pattern of HPV16
sequences into the cellular genome, but expressed similar patterns of
viral messages. Sublines able to grow in the absence of growth
factors (epidermal growth factor and bovine pituitary extract), and
others which became resistant to differentiation stimuli (serum and
calcium) were obtained by selection in growth factor-free medium and
serum-supplemented medium, respectively. The establishment of
continuous cell lines is a direct consequence of the presence of
viral sequences; however, because none of these lines formed tumors
in nude mice, additional events must be necessary for progression of
malignancy. HPV16-immortalized human keratinocyte lines can be used
to investigate and identify the viral factors involved with the
modification of growth and differentiation control by
HPV16.
50. Woodworth CD, Bowden PE, Doniger J, et al.: Characterization
of normal human exocervical epithelial cells immortalized in vitro by
papillomavirus types 16 and 18 DNA. Cancer Res 48:4620-4628, 1988.
An in vitro system for studying the interaction between human
papillomavirus (HPV) 16 and 18 recombinant DNA and normal human
exocervical epithelial cells is described. Eight HPV-immortalized
human exocervical epithelial cell lines were established; all the
lines contained either integrated HPV16 or 18 sequences and expressed
HPV mRNAs. Thus, integration and expression appear to be required for
immortalization. Immortalized cells (greater than 200 population
doublings to date) divided rapidly (doubling time of 30 to 46 h) and
morphologically resembled primary cultures of normal human
exocervical epithelial cells. They expressed a keratin pattern
consistent with their origin from exocervical epithelium. When
cultured at high density or in the presence of serum they terminally
differentiated. Sublines resistant to terminal differentiation were
selected by growth in serum-supplemented medium. Keratin pattern
changes suggest they have some properties in common with cervical
squamous carcinoma cells. However, HPV-immortalized cell lines were
not tumorgenic in nude mice. Thus, HPV16/18 is not carcinogenic by
itself. These cell lines represent an appropriate model for studying
factors that regulate HPV gene expression in normal cervical
epithelial cells and examining the influence of cocarcinogens on
neoplastic progression.
51. Woodworth CD, Doniger J, DiPaolo JA:
Immortalization of human foreskin keratinocytes by various human
papillomavirus DNAs corresponds to their association with cervical
carcinoma. J Virol 63(1):159-164, 1989. Normal human foreskin
keratinocytes cotransfected with the neomycin resistance gene and
recombinant human papillomavirus (HPV) DNAs (types 16, 18, 31, and
33) that have a high or moderate association with cervical malignancy
acquired immortality and contained integrated and transcriptionally
active viral genomes. Only transcripts from the intact E6 and E7
genes were detected in at least one cell line, suggesting that one or
both of these genes are responsible for immortalization. Recombinant
HPV DNAs with low or no oncogenic potential for cervical cancer
(HPV1a, -5, -6b, and -11) induced small G418-resistant colonies that
senesced as did the nontransfected cells. These colonies contained
only episomal virus DNA; therefore, integration of HPV sequences is
important for immortalization of keratinocytes. This study suggests
that the virus-encoded immortalization function contributes to the
pathogenesis of cervical carcinoma.
52. Guido MC, Zamorano R, Garrido-Guerrero E, et
al.: Early promoters of genital and cutaneous human papillomaviruses
are differentially regulated by the bovine papillomavirus type 1 E2
gene product. J Gen Virol 73(Pt 6):1395-1400, 1992. The physical
state of the human papillomavirus (HPV) genome is usually different
in malignant lesions of the skin, in which it is generally found in
episomal form, and genital mucosa, in which it is frequently
integrated with disruption of the E2 gene. Using chimeric or natural
HPV promoters in the presence of the bovine papillomavirus type 1 E2
gene product, we observed transcription activation or repression,
depending on the distance of E2-binding motifs from the start site.
We found a clear difference in the positions of E2-binding motifs in
cutaneous and genital HPVs that may partly explain the selective
pressure for genome integration of genital HPV types in malignant
lesions.
53. Swan DC, Vernon SD, Icenogle JP: Cellular proteins involved in
papillomavirus-induced transformation. Arch Virol 138(1-2):105-115,
1994. Human papillomaviruses (HPVs) are associated with at least
80% of cervical carcinomas and are classified as high-risk or
low-risk based on whether or not they are commonly found in cervical
cancers. The high-risk HPVs have early gene products (E6 and E7) that
immortalize human keratinocytes and are at least partially
responsible for causing cervical carcinoma. E6 and E7 from the
high-risk viruses interact strongly with the tumor suppressors p53
and Rb; those from the low-risk HPVs do not. Transformation involves
a multi-step process and requires additional factors besides
high-risk HPV infection. High-risk HPVs are capable of immortalizing
primary human keratinocytes in tissue culture, but such cells become
transformed only after certain chromosomal changes take place,
possibly having to do with oncogene activation. The DNA of high-risk
HPVs is frequently (if not always) integrated into the genome of
cancer cells; it is normally episomal in premalignant lesions.
Integration disrupts the E2 and E5 genes and viral gene regulation.
Cells containing integrated viral DNA show excessively high levels of
E6 and E7. While there is some conflicting evidence, it appears that
the p53 and Rb tumor-suppressor genes are more frequently mutated in
HPV-negative tumors than they are in HPV-positive tumors, suggesting
that for tumor formation to proceed the p53 and Rb proteins must be
inactivated either by interaction with the viral proteins or by
mutation. The presence of an activated oncogene in a cell lacking
functional p53 or Rb may then be sufficient to cause tumor
progression. [References: 67]
54. Jeon S, Allen-Hoffmann BL, Lambert PF:
Integration of human papillomavirus type 16 into the human genome
correlates with a selective growth advantage of cells. J Virol
69(5):2989-2997, 1995. Integration of human papillomavirus type
16 (HPV-16) DNA into a host chromosome has been hypothesized to
result in altered expression of two viral transforming genes, E6 and
E7, in cervical cancers. In order to investigate the role that
changes in viral genomic state and gene expression play in cervical
carcinogenesis, we have derived clonal populations of human cervical
epithelial cells which harbor multiple copies of either
extrachromosomal or integrated viral DNA. The clonal populations
harboring extrachromosomal HPV-16 DNA stably maintained approximately
1,000 viral copies for at least 15 passages (approximately 100 cell
doublings), which contrasted with the unstable HPV-16 replicons in
the parental counterpart. In the clonal populations harboring
integrated viral DNA, 3 to 60 copies of HPV-16 DNA were found
integrated in either of two forms: type 1, in which all the copies of
HPV-16 DNA were disrupted in the E2 open reading frame upon
integration, and type 2, in which intact viral copies were flanked by
disrupted viral copies and cellular sequences. Despite the lower
HPV-16 DNA copy number, the clonal populations with integrated viral
DNA had levels of E7 protein that were in most cases higher than
those found in the clonal populations harboring extrachromosomal
viral DNA. Irrespective of viral genomic state, the clonal
populations were capable of undergoing terminal differentiation and
unable to form colonies in soft agar, which is indicative of the
nontumorigenic nature of these cells. Importantly, a cell population
with integrated viral DNA was found to outgrow another with
extrachromosomal DNA when these cells were cocultured over a period
of time. Thus, integration of human papillomaviral DNA correlates
with increased viral gene expression and cellular growth advantage.
These observations are consistent with the hypothesis that
integration provides a selective advantage to cervical epithelial
precursors of cervical carcinoma.
55. Chen SL, Tsao YP, Lee JW, et al.:
Characterization and analysis of human papillomaviruses of skin
warts. Arch Dermatol Res 285(8):460-465, 1993. We analysed human
papillomavirus (HPV) infections in 61 tissue specimens of skin warts
of Taiwanese patients by DNA hybridization. The prevalence of HPV
infection was 69% by Southern blot hybridization. The typing of HPVs
was performed by dot blot hybridization under highly stringent
conditions with each probe separately. The prevalence of HPV-1, 2/3,
4, 5, 8, 11, 16 and 18 in skin warts was 13, 7, 16, 2, 0, 5, 2 and
8%, respectively. Chi-squared analysis revealed that there was a
correlation between HPV type and copy number. Most HPV-4-induced
warts were verruca vulgaris. HPV-1 DNA was detected in verruca
plantaris and verruca vulgaris. No specific histopathological
features were found to be indicative of the presence or absence of
HPV, or of the various types of HPV infection.
56. Kienzler JL, Lemoine MT, Orth G, et al.:
Humoral and cell-mediated immunity to human papillomavirus type 1
(HPV-1) in human warts. Br J Dermatol 108(6):665-672, 1983. The
humoral and cell-mediated immune response to human papillomavirus
type 1 (HPV-1) has been studied in 162 patients carrying papillomas
of various clinical types: deep plantar wart or myrmecia, common
wart, flat wart, and anogenital wart. Circulating antibodies were
detected by immunodiffusion and microcomplement fixation, using
purified HPV-1 particles as type-specific antigen. A significant
association between myrmecia and anti-HPV-1 antibodies was found (39%
of the cases). Cell-mediated immunity was evaluated by a study of
delayed hypersensitivity (DH). The main capsid components of HPV-1
(HPV-1 CP), consisting mostly of a polypeptide of molecular weight
54,000, were injected intradermally. In addition to the type-specific
antigens, HPV-1 CP contain other antigenic determinants shared by
various types of human papilloma-viruses and masked in intact viral
particles. The DH tests to HPV-1 CP showed no differences between the
carriers of different papilloma types, confirming the presence of
common antigenic determinants. Moreover, they gave rise to an
increase or to new anti-HPV-1 antibody production mostly in myrmecia
carriers (78% and 33% of the cases, respectively), and to new DH to
HPV-1 CP in all groups of papilloma carriers (33% to 56%, depending
on the clinical papilloma type).
57. Jablonska S, Obalek S, Favre M, et al.: The
morphology of butchers' warts as related to papillomavirus types.
Arch Dermatol Res 279(Suppl):S66-72, 1987. Hand warts were
studied in 160 butchers. Clinical and histological studies were
performed in 190 warts and virological studies in 165 warts from 104
butchers. Since we found almost perfect correlation between the
histological pattern and the type of infecting virus, it was possible
to evaluate the virus types in a further 39 of 56 butchers without
virological studies, on the basis of the histology of the warts. The
most common infection was with HPV-2 (human papilloma virus) and
HPV-7. Thirty-three butchers were infected with two types of viruses
and three butchers with three HPVs. The morphology of warts varied
considerably. The majority were similar to verrucae vulgares or
verrucae planae. Some deep warts resembled myrmecia-type verrucae
plantares. Often, several types of warts coexisted. Some clinical
patterns were shown to be preferentially associated with distinct
types of papillomaviruses: common warts with HPV-2, HPV-4, or HPV-7,
plane and intermediate warts with HPV-3, HPV-10, HPV-28. HPV-7,
previously identified for the first time in these butchers, was found
to be associated with common warts or common wart-like, papillomatous
lesions.
58. Jacyk WK, De Villiers EM: Epidermodysplasia verruciformis in
Africans. Int J Dermatol 32(11):806-810, 1993. BACKGROUND.
Epidermodysplasia verruciformis (EV) is a rare cutaneous disorder
characterised by persistent, refractory infection with human
papillomaviruses (HPV). Although EV does not seem to have racial or
geographic preference, there is a scarcity of reports on its
occurrence in Africans. METHODS. Twenty Africans with EV were
studied, and the literature on this condition in Africans was
reviewed. Virologic studies were performed on 10 patients. RESULTS.
Three types of lesions were observed: flat warts, pityriasis
versicolor-like macules, and seborrheic keratosis-like changes.
Malignant transformation occurred in only one patient. HPV-3 was
isolated only from flat warts, HPV-5 and HPV-17 were isolated only
from PV-like lesions, whereas an HPV-5-related type was found in all
three types of changes. HPV-5-related type revealed DNA that was
related but not identical to any of the viruses in the HPV-5 group.
This particular type was isolated from all five South African
patients with EV in whom virologic studies were performed.
CONCLUSIONS. The benign nature of EV in dark-skinned Africans has
been confirmed. Four HPV types have been isolated, of which
HPV-related type was found in all South African patients with EV and
in all types of skin changes, regardless of their morphology. African
patients with EV frequently present seborrheic keratosis-like
changes.
59. Kanda R, Tanigaki T, Kitano Y, et al.: Types
of human papillomavirus isolated from Japanese patients with
epidermodysplasia verruciformis. Br J Dermatol 121(4):463-469, 1989.
Virological studies were performed on 12 patients with
epidermodysplasia verruciformis (EV). Three types of lesions were
observed: red plaques, pityriasis versicolor (PV)-like macules and
plane warts. Human papillomavirus (HPV) 14, 20 and 21 were isolated
from the plaques, HPV 3, 14 and 38 from flat warts and HPV 5, 12, 17,
20 and 38 from PV-like lesions. No clear relationship could be
established between the different lesions and the types of HPV. Types
17 and 20 have been isolated most frequently from Japanese EV
patients and HPV 5, frequently detected in other countries, is less
common, whereas HPV 8 has not been isolated. Skin cancers occurred in
six of the cases (50%) and all had benign lesions that were PV-like.
At least one type of HPV 5, 17 or 20 could be isolated from these
benign lesions and HPV 17 or 20 detected in the cancers. These three
types of HPV in EV patients appear to be involved in the malignant
transformation. Author-abstract
60. Ostrow RS, Manias D, Mitchell AJ, et al.: Epidermodysplasia
verruciformis. A case associated with primary lymphatic dysplasia,
depressed cell-mediated immunity, and Bowen's disease containing
human papillomavirus 16 DNA. Arch Dermatol 123(11):1511-6, 1987.
Epidermodysplasia verruciformis is a rare, often hereditary
disease characterized by a generalized cutaneous infection with human
papillomavirus (HPV), depressed cell-mediated immunity, and a
propensity for transformation of the warty lesions to squamous cell
carcinoma on primarily sun-exposed areas of the skin. A 37-year-old
man with congenital lymphatic dysplasia and a history of squamous
cell carcinoma of the groin and foot was observed by us to have edema
of all four extremities, numerous flat warts, and pityriasis
versicolor-like papules over the trunk and arms. Condylomatous
lesions were noted in the groin and a periungual verrucous nodule on
the thumb. Biopsies showed the trunk and arm lesions to be verrucae
and the thumb lesion to be Bowen's disease. Results of molecular
hybridization studies from four lesions of the arms showed the
presence of only HPV 3 DNA; HPV 16-related DNA was detected in the
intraepidermal carcinoma on the thumb. Immunologic evaluation
revealed anergy to routine skin testing, depressed mitogen-stimulated
lymphocyte transformation, decreased B-lymphocyte count, and a severe
reversal of the T-lymphocyte helper:suppressor ratio.
Author-abstract
61. Kremsdorf D, Jablonska S, Favre M, et al.:
Human papillomaviruses associated with epidermodysplasia
verruciformis. II. Molecular cloning and biochemical characterization
of human papillomavirus 3a, 8, 10, and 12 genomes. J Virol
48(2):340-351, 1983. The DNAs of four human papillomaviruses
(HPVs) that were found in the benign lesions of three patients
suffering from epidermodysplasia verruciformis have been
characterized. The flat wart-like lesions and the macular lesions of
patient 1 contained two viruses, HPV-3a and HPV-8, respectively,
whose genomes had previously been only partially characterized. The
flat wart-like lesions of patient 2 and the macular lesions of
patient 3 each contained a virus previously considered as belonging
to types 3 and 5, respectively. These viruses are shown in the
present study to be different from all of the HPV types so far
characterized; they have tentatively been named HPV-10 and HPV-12.
The HPV-3a, HPV-8, and HPV-12 DNAs and the two SalI fragments of
HPV-10 DNA (94.1 and 5.9% of the genome length) were cloned in
Escherichia coli after having been inserted in plasmid pBR322. The
cloned HPV genomes have similar sizes (about 7,700 base pairs), but
their guanine-plus-cytosine contents differ from 41.8% for HPV-12 DNA
to 45.5% for HPV-3a DNA. The study of the sensitivity of the four HPV
DNAs to 14 restriction endonucleases permitted the construction of
cleavage maps. Evidence for conserved restriction sites was found
only for the HPV-3a and HPV-10 genomes since 5 of the 21 restriction
sites localized in the HPV-3a DNA seem to be present also in the
HPV-10 DNA. Hybridization experiments, performed in liquid phase at
saturation, showed a 35% sequence homology between HPV-3a and HPV-10
DNAs, 17 to 29% sequence homology among HPV-5, HPV-8, and HPV-12
DNAs, almost no sequence homology between the HPV-3a or HPV-10 DNA
and the other HPV DNAs, and a weak homology between HPV-9 DNA and
HPV-8 or HPV-12 DNA. Blot hybridization experiments showed no
sequence homology between the HPV-3a, HPV-8, and HPV-12 DNAs and the
DNAs of the HPVs associated with skin warts (HPV-1a, HPV-2, HPV-4,
and HPV-7) or with mucocutaneous and mucous membrane lesions (HPV-6b
and HPV-11a, respectively). One exception was a weak sequence
homology between the HPV-2 prototype and HPV-3a or HPV-10
DNA.(ABSTRACT TRUNCATED AT 400 WORDS)
62. Ostrow R, Zachow K, Watts S, et al.: Characterization of two
HPV-3 related papillomaviruses from common warts that are distinct
clinically from flat warts or epidermodysplasia verruciformis. J
Invest Dermatol 80(5):436-440, 1983. We have recently identified
two unusual human papillomavirus (HPV) isolates while engaged in an
ongoing study of wart disease in meat handlers and veterinarians. The
papillomas from which these two viruses were isolated clinically
resembled verruca vulgaris rather than either flat warts or
epidermodysplasia verruciformis (EV). These two previously
uncharacterized HPVs were molecularly cloned and characterized with
respect to known HPVs. The genomes of the two viruses exhibited
dramatically different restriction endonuclease cleavage patterns but
were found to have significant sequence homology to each other, as
well as to HPV-3 and a new virus isolated from a patient with EV.
Neither of the two new HPV isolates exhibit detectable sequence
homology under stringent conditions of hybridization or share similar
restriction endonuclease cleavage patterns with previously
characterized HPV types 1,2,4,5,6b, or a previously isolated HPV from
meat handlers.
63. Pfister H: Human papillomaviruses and skin
cancer. Semin Cancer Biol 3(5):263-271, 1992. Human
papillomavirus (HPV)-induced skin warts are classically benign
lesions. However an association between specific HPV types and skin
cancer becomes obvious in epidermodysplasia verruciformis (EV). The
analysis of this disease suggests that lesions infected with HPV
types 5 and 8 carry a high risk of developing squamous cell
carcinomas. The oncogenes of EV-viruses appear to be E6 and E2,
rather than E7. The 'high risk' EV-viruses, HPV 5, 8, and 47, differ
from related HPV types in the transforming activity of the E6 gene
and in the density of positive transcription control elements in the
non-coding region (NCR) of the genome. The extrachromosomal viral DNA
in cancers may show deletions affecting regulatory sequences.
EV-specific lesions occasionally occur in immunosuppressed patients
and HPV 5 or 8 persist in some of the skin cancers to which these
patients are prone. DNAs of HPV 2, 16, 34, or 41 were identified in
few premalignant and malignant skin tumors of the general population.
[References: 65]
64. Melchers W, de Mare S, Kuitert E, et al.:
Human papillomavirus and cutaneous warts in meat handlers. J Clin
Microbiol 31(9):2547-2549, 1993. The association of
papillomavirus and hand warts in meat handlers was examined. Human
papillomavirus (HPV) DNA was found in 23 (88%) of 26 cutaneous warts,
with HPV 7 (27%) and a yet unidentified HPV (HPV X) (42%) being the
predominant types. HPV 2 was found in two (7.5%) patients, and HPV 4
was found in three (11.5%) patients. No bovine papillomavirus
sequences were detected. In most patients, the warts developed in
less than 2 years after they started working with meat. A possible
HPV transmission route by protection gloves and professional
equipment is suggested.
65. Jablonska S, Obalek S, Golebiowska A, et
al.: Epidemiology of butchers' warts. Arch Dermatol Res
280(Suppl):S24-S28, 1988. Studies were carried out in two
slaughter-houses in different cities differing in the degree of work
automation and, for comparison, in workers of nearby factories of the
same two cities. There was a high incidence of warts (49.2%) in a
slaughterhouse where the workers had direct contact with animals and
meat, while a significantly lower incidence (9%) was observed in a
modern slaughterhouse where the work was almost completely automated.
The types of human papillomaviruses (HPVs) were similar in warts of
butchers from these slaughterhouses and of 63 butchers from various
slaughterhouses all over the country. All cutaneous HPVs were present
in butchers' warts. The so-called butchers' wart virus HPV-7 was
found in about 30% of the butchers from all slaughterhouses.
Cell-mediated immunity of the butchers was found to be unimpaired.
There was no correlation between the incidence of infection and the
frequency of antibodies against HPV-1, HPV-2, or HPV-3.
66. Kremsdorf D, Jablonska S, Favre M, et al.:
Biochemical characterization of two types of human papillomaviruses
associated with epidermodysplasia verruciformis. J Virol
43(2):436-447, 1982. The DNAs of the human papillomaviruses
(HPVs) associated with the benign lesions of two patients suffering
from epidermodysplasia verruciformis (patients JD and JK) were
analyzed by using 12 restriction endonucleases. None of the
restriction endonucleases were one-cut enzymes for the HPV DNA
obtained from patient JD, referred to as the prototypical HPV-5,
whereas five of them were one-cut enzymes for the DNA of the major
virus found in patient JK, referred to as HPV-9. The molecular
cloning of the two fragments resulting from the cleavage of HPV-5 DNA
by endonuclease HindIII and of the single fragment obtained after
treatment of HPV-9 DNA with endonuclease BamHI was performed in
Escherichia coli after the fragments were inserted in plasmid pBR322.
A cleavage map of the two cloned genomes was constructed. Little
sequence homology (4 to 5%) was detected between HPV-5 and HPV-9 DNAs
by DNA-DNA hybridization experiments in liquid phase at saturation;
this homology was reproducibly higher than that (2 to 3%) detected
under the same conditions between these DNAs and HPV-1a DNA. In
addition, blot hybridization experiments performed under stringent
conditions showed no or little sequence homology between the DNAs of
HPV-5 and HPV-9 and those of HPV prototypes of types 1, 2, 3, 4, and
7 associated with skin warts. These results confirm that HPV-5 and
HPV-9 are two distinct HPV types.
67. Ficarra G, Adler-Storthz K, Galeotti F, et
al.: Focal epithelial hyperplasia (Heck's disease): the first
reported case from Italy. Tumori 77(1):83-85, 1991. A case of
focal epithelial hyperplasia (Heck's disease) of the oral mucosa
observed for the first time in Italy is reported. The patient was of
Italian extraction. The lesions, represented by soft nodules, were
multiple and located on the vestibular and labial mucosa. Biopsy
tissues were studied for the presence of human papilloma virus (HPV)
by electron microscopy, in situ hybridization and immunoperoxidase
staining to HPV group antigens. No viral particles consistent with
HPV were found in the epithelial cells. The tissues were positive for
HPV antigen by immunoperoxidase staining and hybridized to the HPV 13
probe. In situ hybridization to the HPV 6, HPV 11, HPV 16, HPV 18 and
32 probes was negative. Our study substantiates that focal epithelial
hyperplasia, although rare, may be observed in Whites and that HPV 13
in associated with the disease.
68. Williamson AL, Dennis SJ: The use of the
polymerase chain reaction for the detection of human papillomavirus
type 13. J Virol Methods 31(1):57-65, 1991. Human papillomavirus
type 13 (HPV-13) is associated with oral focal epithelial hyperplasia
(FEH). The purpose of this study was to establish conditions for the
application of polymerase chain reaction (PCR) to the specific
detection and amplification of HPV-13 DNA. To design primers for
HPV-13 a part of the HPV-13 genome was sequenced first: the smallest
BamHI fragment (597 bp) of HPV-13 was subcloned and sequenced. The
sequence was found to be part of a large open reading frame and had
significant homology with the L1 gene of other HPVs. HPV-13 specific
primers were designed to amplify a 240 bp fragment from the L1 gene
by PCR. Conditions for PCR were standardized for this set of
primers.
69. Henke RP, Guerin-Reverchon I, Milde-Langosch K, et al.: In
situ detection of human papillomavirus types 13 and 32 in focal
epithelial hyperplasia of the oral mucosa. J Oral Pathol Med
18(7):419-421, 1989. 17 cases of focal epithelial hyperplasia of
the oral mucosa (FEH, Heck's disease) were investigated for the
presence of human papillomavirus (HPV) nucleic acid sequences by
means of in situ DNA hybridization using biotinylated DNA probes of
HPV types 1, 6, 11, 13, 16, 18, and 32. Ten of 17 cases were positive
for HPV 13 DNA in contrast to 6 of 17 positive cases obtained after
application of the HPV 32 probe, with a double infection in one case.
The results of our study suggest, that HPV 13 and HPV 32 are very
specifically found in lesions of FEH and can be detected in a high
percentage of cases using in situ hybridization.
70. Garlick JA, Calderon S, Buchner A, et al.:
Detection of human papillomavirus (HPV) DNA in focal epithelial
hyperplasia. J Oral Pathol Med 18(3):172-177, 1989. Five focal
epithelial hyperplasia (FEH) specimens from four patients were
examined by Southern blot hybridization analysis to determine the
specific human papillomavirus (HPV) types present. The
histomorphologic features of these specimens were also evaluated and
a broad variety of changes including koilocytes, mitosoid cells,
ballooning cells and cells showing individual cell keratinization
were noted. FEH lesions from the three patients sharing a familial
relationship demonstrated HPV DNA sequences that were either the
prototype HPV-13 or a very closely related HPV-13 subtype. These
patients also showed similar clinical features. Lesional tissue from
the other patient was found to harbor HPV DNA sequences similar to
HPV-32. In view of these findings it is suggested that these specific
HPV types are associated with the characteristic FEH histomorphology
described.
71. Henke RP, Milde-Langosch K, Loning T, et al.: Human
papillomavirus type 13 and focal epithelial hyperplasia of the oral
mucosa: DNA hybridization on paraffin-embedded specimens. Virchows
Arch A Pathol Anat Histopathol 411(2):193-198, 1987. 16 cases of
focal epithelial hyperplasia (Heck's disease) were studied for the
presence of human papillomavirus DNA by means of nucleic acid
hybridization. Hybridization was carried out in situ with
biotin-labelled probes of HPV 1, 6, 11, 13, 16, and 18 DNA under
stringent and non-stringent conditions. Under non-stringent
conditions, 6 of 16 cases (38%) hybridized to a mixture of HPV 1, 6,
11, 16, and 18 DNA. When these probes were applied under stringent
conditions, only one case could be shown to be weakly positive for
HPV 6/11 DNA. Further stringent hybridizations, which were conducted
with a HPV 13 probe on 12 of our 16 cases, revealed a positive result
in 9 of 12 cases (75%). The results of our study strongly
substantiate the concept that HPV 13 or a closely related HPV type is
associated with lesions morphologically presenting as focal
epithelial hyperplasia.
72. Hernandez-Jauregui P, Eriksson A, Tamayo Perez R, et al.:
Human papillomavirus type 13 DNA in focal epithelial hyperplasia
among Mexicans. Brief report. Arch Virol 93(1-2):131-137, 1987.
Human papillomavirus (HPV) type 13 DNA was detected in focal
epithelial hyperplasia lesions of the oral mucosa in seven half-caste
mexicans. The lesions contained intracellular papillomavirus-like
particles with a diameter of about 50 nm. DNA extracted from biopsies
contained unintegrated HPV type 13 DNA genomes as revealed by
Southern blot hybridization. The HPV 13 DNA that was isolated in the
present study had the same restriction enzyme cleavage map as HPV 13
DNA, previously described by others. It was moreover confirmed that
HPV type 13 genome is related to the genomes of HPV types 6 and
11.
73. Lutzner MA, Blanchet-Bardon C, Orth G:
Clinical observations, virologic studies, and treatment trials in
patients with epidermodysplasia verruciformis, a disease induced by
specific human papillomaviruses. J Invest Dermatol 83(1
Suppl):18s-25s, 1984. We have studied 11 patients with the
papillomavirus-induced disease epidermodysplasia verruciformis (EV).
Clinical diagnostic features are widespread, long-lasting, pityriasis
versicolor-like macules and flat, wart-like papules, both usually
occurring in early childhood, with the subsequent development in the
third decade of multiple skin cancers of the Bowenoid in situ and
squamous cell types, primarily in sun-exposed skin. Virologic studies
using the methods of immunofluorescence microscopy, restriction
endonuclease analysis, and DNA blot hybridization have shown benign
lesions to be associated with one or several types of the human
papillomaviruses (HPVs) specifically associated with EV (at least 15
types recognized on the basis of sequence homology studies of
molecularly cloned genomes). Skin cancers in these patients were
associated with the genomes of either HPV-5, HPV-8 or HPV-14,
suggesting that these three viruses are potentially oncogenic. A
genetic factor appears to play a role in the pathogenesis of EV,
since 5 of our patients were children of consanguineous parents and 2
had siblings also suffering with EV, suggesting a recessive
inheritance pattern. Treatment of 4 EV patients with an oral retinoid
resulted in partial temporary improvement of benign lesions, and the
treatment of 2 patients with intralesional interferon injections into
multiple Bowenoid cancers in situ has resulted in the disappearance
of these lesions. Finally, EV serves as a model for studying the
interplay of oncogenic viruses, genetic and immunologic factors, and
sunlight in the production of skin cancer in humans.
74. Lutzner MA: Papillomaviruses and skin cancer
in Africa. IARC Sci Publ (63):607-623, 1984. Although it was
suggested long ago that certain epithelial cancers preceded by
papillomas might be caused by viruses, the first proof that
papillomaviruses were associated with cancer dates from the work on
rabbits in 1934 by Shope and Rose. In the 1970s, the introduction of
the blot hybridization technique enabled Orth and his co-workers at
the Institut Pasteur, Paris, to demonstrate the presence in man of
the DNA of human papillomavirus type 5 (HPV-5) in cancers following
Lutz-Lewandovsky epidermodysplasia verruciformis. Some years later,
it was possible to demonstrate the presence of the same HPV-5 DNA in
the skin cancer of an immunosuppressed recipient of a renal
transplant. The number of potentially oncogenic papillomaviruses has
recently been increased by the demonstration at the Institut Pasteur
of the presence of the DNAs of HPV-8 and HPV-14 in the skin cancers
of patients with epidermodysplasia verruciformis. In recent years, an
association has been demonstrated between HPV-6, -10, -11, -16, and
-18 with verrucous cancers of the skin and mucous membranes, Bowenoid
papules, Bowenoid skin diseases and cervical cancer. Such cancers of
the skin and mucous membranes are usually treated by surgery, but it
has been shown that oral administration of retinoids (synthetic
derivatives of vitamin A) or the use of leucocyte interferon
intralesionally are effective in cancers in situ following
epidermodysplasia verruciformis.
75. Bergeron C, Barrasso R, Beaudenon S, et al.:
Human papillomaviruses associated with cervical intraepithelial
neoplasia. Great diversity and distinct distribution in low- and
high-grade lesions. Am J Surg Pathol 16(7):641-649, 1992. All
together, 30 genital human papillomavirus (HPV) types have been
characterized so far. To evaluate the importance of HPV diversity in
associated cervical diseases, we analyzed 188 biopsy specimens
obtained from patients with a recent diagnosis of cervical HPV
infection or intraepithelial neoplasia (CIN). Of these 188 specimens,
116 were classified as low-grade CIN (48 cases), high-grade CIN (53
cases), condylomata acuminata (10 cases), flat condylomas (five
cases). Seventy-two specimens were considered nondiagnostic. Using
probes specific for 18 genital HPV types, HPV DNA sequences were
detected by Southern blot hybridization in 100 lesions and 21
nondiagnostic specimens. When further analyzed by the polymerase
chain reaction, eight HPV-negative biopsy specimens, four CIN, and
four nondiagnostic specimens were positive. Of the 129 positive
biopsy specimens, 92 contained at least one of 18 known HPV types and
37 HPV that have not yet been identified. Nine specimens had more
than one type. Thirteen HPV types were identified in CIN. The
detection rate of HPV 16 increased from 21% in low-grade CIN to 57%
in high-grade CIN. HPV 18 was detected in only 3% of CIN; HPV 31, 33,
and 35 were found in 8%. HPV 30, 39, 45, 51, 52, 56, 58, and 61 were
detected in 44% of low-grade CIN but in only 8% of high-grade CIN.
Unidentified HPV were detected in about 25% of low-grade and
high-grade CIN. Fifty-seven CIN positive for at least one HPV type
were further analyzed by in situ hybridization. Thirty-five (65%)
biopsy specimens were positive, including 21 of 24 low-grade CIN and
14 of 33 high-grade CIN. Ten of the 13 previously identified HPV
types were detected. Thus, CIN represents an heterogeneous disease
from a virologic viewpoint. This fact could explain their variable
clinical evolution.
76. Gassenmaier A, Pfister H, Hornstein OP:
Human papillomavirus 25-related DNA in solitary keratoacanthoma. Arch
Dermatol Res 279(2):73-76, 1986. Solitary keratoacanthomas of 32
patients were screened for the presence of human papillomavirus (HPV)
25 DNA, which was originally isolated and molecularly cloned from
warts of an epidermodysplasia verruciformis (Ev) patient.
Biotinylated virus DNA was hybridized in situ to thin sections
obtained from paraffin-embedded material. HPV DNA was detected in 12
of 32 tumors under stringent conditions, and in 2 additional tumors
under relaxed conditions.
77. Payne D, Chan TS, Wagner R, et al.: Cloning
of mucosal and cutaneous HPV sequences in a metastatic squamous cell
carcinoma from an epidermodysplasia verruciformis patient. Anticancer
Res 16(3A):1165-1166, 1996. Human papillomavirus (HPV) is a DNA
tumor virus strongly associated with cervical neoplasias. There are
over 80 different types of HPVs which can infect either mucosal or
cutaneous tissue. Cutaneous squamous cell carcinomas (SCC) associated
with HPV are often seen in patients with epidermodysplasia
verruciformis (EV). EV is characterized by cutaneous lesions that
progress to SCC upon UV exposure. In characterizing the HPV types
associated with an unusually aggressive form of EV, we have cloned an
HPV with homology to the moderately oncogenic genital type HPV 34,
the oncogenic EV type HPV 5 and from benign oral mucosal type HPV 32.
The presence of sequences from these highly divergent types is a
novel finding. These three viral types are from different
phylogenetic branches of the HPV family believed to have evolved
independently from each other.
78. Kawashima M, Favre M, Obalek S, et al.:
Premalignant lesions and cancers of the skin in the general
population: evaluation of the role of human papillomaviruses. J
Invest Dermatol 95(5):537-542, 1990. To evaluate the role of
human papillomaviruses (HPV) in the development of premalignant
lesions and cancers of the skin in the general population, 314
biopsies obtained from 227 patients with benign neoplasms,
premalignant lesions, and cancers of the skin and from 25 patients
with squamous cell carcinoma of the lip were analyzed by Southern
blot hybridization. DNA probes specific for various cutaneous and
genital HPV types were used in hybridizations conducted under
nonstringent or stringent conditions. HPV DNA sequences were only
detected in eight specimens obtained from six patients: HPV 34 in one
case of periungual Bowen's disease, HPV 36 and an as yet
uncharacterized HPV in two cases of actinic keratosis, HPV 20 in one
case of basal cell carcinoma, an as yet unrecognized HPV in one case
of squamous cell carcinoma, and HPV 16 in one case of squamous cell
carcinoma of the lip. None of the specimens of cutaneous horn and
keratoacanthoma contained detectable HPV DNA. In contrast, HPV DNA
sequences, mostly HPV 16, were detected in 13 of 23 cases of
anogenital Bowen's disease and invasive Bowen's carcinoma. HPV DNA
sequences were not detected in 90 cutaneous samples further analyzed
by the polymerase chain-reaction technique, using amplification
primers that contain conserved sequences among the genomes of HPV.
These results strongly suggest that the known HPV types play only a
minor role, if any, in skin carcinogenesis in the general population.
Author-abstract
79. Scheurlen W, Gissmann L, Gross G, et al.:
Molecular cloning of two new HPV types (HPV 37 and HPV 38) from a
keratoacanthoma and a malignant melanoma. Int J Cancer 37(4):505-510,
1986. Several benign and malignant skin tumors were analyzed for
the presence of human papillomavirus (HPV) DNA. By hybridization with
different HPV DNA probes under non-stringent conditions (Tm -40
degrees C), two tumors were found to contain HPV-specific DNA
sequences in high copy numbers: (1) a keratoacanthoma from a patient
who also suffered from a basalioma; (2) a superficial spreading
malignant melanoma of an immunosuppressed patient. For further
analysis of these DNA sequences genomic libraries from both tumor
DNAs were constructed and, out of these, 4 different HPV DNA types
have been cloned. By cross-hybridization experiments and restriction
map analysis HPV 9 DNA was identified in the keratoacanthoma whereas
HPV 17a DNA could be cloned from the malignant melanoma. From each
tumor one additional HPV-type not identical to other known HPV-types
was cloned. These isolates are closely related to HPV 9, 15, 17, 22
and 23. A physical map of both HPV DNAs was constructed. Size (7.8
kbp), co-linear alignment to HPV 16, cross-hybridization with other
HPV-types under conditions of low stringency and monomeric episomal
state of the HPV molecules indicate that these two DNA probes
represent new HPV types that have been tentatively designated as HPV
37 (keratoacanthoma) and HPV 38 (malignant melanoma). None of these
two HPV types could be found in any other of 231 tumor DNAs
originating from different tissues. Author-abstract
80. Yutsudo M, Kanda R, Tanigaki T, et al.:
Human papillomavirus type 38 isolated from patients with
epidermodysplasia verruciformis. Intervirology 26(1-2):104-108,
1986. A new type of human papillomavirus (HPV), HPV-38b, was
isolated from patients with epidermodysplasia verruciformis and was
molecularly cloned. This HPV was shown by hybridization experiments
to have almost no sequence homology with other types of reported
HPVs, but did show homology with HPV-38, which was recently isolated
from a melanoma. A physical map and a rough genetic map of the
organization of this HPV are presented.
81. Joste NE, Rushing L, Granados R, et al.:
Bethesda classification of cervicovaginal smears: reproducibility and
viral correlates. Hum Pathol 27(6):581-585, 1996. Fifty-five
cervicovaginal smears from women with squamous intraepithelial
lesions (SILs) were independently evaluated on two separate occasions
by four cytopathologists using a binary classification system (the
Bethesda system). Smears were categorized as low-grade (LSIL) or
high-grade (HSIL) using previously published criteria. All women had
subsequent cervical biopsies containing human papillomavirus (HPV)
DNA amplified with the polymerase chain reaction and typed by
restriction fragment polymorphism analysis. Three or more observers
agreed on classification in 49 of 55 cases (87%); unanimous diagnoses
were rendered in 31 cases (56%). Interobserver and intraobserver
reproducibility ranged from fair to near-excellent (kappa values 0.40
to 0.63; 0.63 to 0.74, respectively). HPV types included HPV 16
(27%), 18 (7%), 31 (9%), 35 (4%), 39 (4%), 6 (10%), 11 (2%), novel
types (30%), and multiple types (4%). High-risk HPV types (16, 18,
31, 35, and 39) were significantly associated (P = .03) with
consensus HSIL diagnoses (agreement of three or more observers). This
was primarily because of the strong association of HPV 16 with HSIL
(P = .001). After excluding HPV 16, the other high-risk HPV types
(18, 31, 35, and 39) were no longer significantly associated with
consensus HSIL diagnoses (P > .5). Conversely, LSIL diagnoses were
significantly associated with non-high-risk HPV types (all HPV types
except 16, 18, 31, 35, and 39; P = .006). Binary cytological
classification of cervicovaginal SILs is reproducible among
cytopathologists. Such classification correlates well with most
low-risk HPV types and with the prototypic high-risk HPV 16 but not
with other high-risk HPV types.
82. de Villiers EM, Hirsch-Behnam A, von
Knebel-Doeberitz C, et al.: Two newly identified human papillomavirus
types (HPV 40 and 57) isolated from mucosal lesions. Virology
171(1):248-253, 1989. Two new papillomaviruses, HPV 40 and HPV
57, were isolated from a PIN lesion and an inverted papilloma of the
maxillary sinus, respectively. HPV 40 showed a 13% homology to HPV 7
by reassociation kinetics and HPV 57 showed a 17% homology to HPV 2
and 25% homology to HPV 27. Hybridization of the DNA of these
papillomaviruses to a wide variety of different tumor biopsies
revealed that HPV 40 was present in a few genital condylomata
acuminata as well as in bowenoid lesions. HPV 57 DNA was present in
an oral wart, a genital condyloma acuminatum, and verrucae vulgares
lesions from two immunosuppressed patients.
83. Hirt L, Hirsch-Behnam A, de Villiers EM:
Nucleotide sequence of human papillomavirus (HPV) type 41: an unusual
HPV type without a typical E2 binding site consensus sequence. Virus
Res 18(2-3):179-189, 1991. The complete nucleotide sequence of
human papillomavirus type 41 (HPV-41) has been determined. HPV-41 was
originally isolated from a facial wart, but its DNA has subsequently
been detected in some skin carcinomas and premalignant keratoses
(Grimmel et al., Int. J. Cancer, 1988, 41, 5-9; de Villiers, Grimmel
and Neumann, unpublished results). The analysis of the cloned HPV-41
nucleic acid reveals that its genome organisation is characteristic
as for other papillomavirus types. Yet, the analysis indicates at the
same time that this virus is most distantly related to all other
types of human-pathogenic papillomaviruses sequenced thus far and
appears to identify HPV-41 as the first member of a new subgroup of
HPV. The overall nucleotide homology to other sequenced HPV types is
below 50%. The closest other HPV type is represented by HPV-18,
sharing 49% identical nucleotides. The typical E2 binding sequence
ACCN6GGT, found in all papillomaviruses analyzed to date, does not
occur in the URR of the HPV-41 genome. Modified E2 binding sequences,
as described for BPV 1 (Li et al., Genes Dev. 1989, 3, 510-526), are
located in the domain proximal to the E6 ORF. These are ACCN6GTT,
AACN6GGT and the two perfect palindromic sequences
AACGAATTCGTT.
84. Grimmel M, de Villiers E-M, Neumann C, et
al.: Characterization of a new human papillomavirus (HPV 41) from
disseminated warts and detection of its DNA in some skin carcinomas.
Int J Cancer 41(1):5-9, 1988. A new human papillomavirus type
(HPV 41), distantly related to known HPV prototypes, was isolated
from a patient with disseminated facial, peri-anal and foot warts
(epidermodysplasia verruciformis was not diagnosed). The viral DNA
was molecularly cloned in 2 BamH1 restriction fragments with sizes of
6.5 kb and 0.98 kb, respectively. The classification of this cloned
DNA as a new type is based on the degree of cross-hybridization with
40 HPV types under conditions of varying stringency. A total of 106
benign and malignant skin lesions, as well as 71 malignant tumours of
different origins, were screened for the presence of HPV-related
sequences. In 2 out of 10 squamous-cell carcinomas and in 1 of 3
arsenic keratoses HPV 41 DNA sequences could be detected.
Author-abstract
85. Lorincz AT, Quinn AP, Goldsborough MD, et
al.: Cloning and partial DNA sequencing of two new human
papillomavirus types associated with condylomas and low-grade
cervical neoplasia. J Virol 63(6):2829-2834, 1989. Using
low-stringency Southern blot analysis and cloning in lambda
bacteriophage, two new human papillomavirus types (HPV-43 and HPV-44)
were identified and their DNAs were cloned from vulvar tissues. The
isolates were characterized by restriction endonuclease mapping and
shown to be new HPV types on the basis of their minimal hybridization
with all other known HPV types at high stringency. Both HPVs are most
closely related to types 6, 11, and 13. HPV-43 did not exhibit any
cross-reactivity with these HPV types at high stringency. HPV-44
showed minimal cross-reactivity to HPV-13, which was in the range of
20 to 25% according to liquid hybridization analysis. The deduced
genomic organization of each of the two new HPVs was colinear with
HPV-6b. Prevalence studies revealed that HPV-43 and HPV-44 together
were found in 6 of 439 normal cervical tissues, in 8 of 195 cervical
intraepithelial neoplasms, but in none of 56 cervical cancers tested
thus far.
86. Kiyono T, Adachi A, Ishibashi M: Genome
organization and taxonomic position of human papillomavirus type 47
inferred from its DNA sequence. Virology 177(1):401-405, 1990.
The complete nucleotide sequence of human papillomavirus type 47
(HPV-47) DNA isolated from the lesion of epidermodysplasia
verruciformis (EV) was determined. The computer-aided comparison of
HPV-47 with other EV-associated viruses using the available sequence
data on them revealed that HPV-47 resembles both HPV-5 and HPV-8 as
much as HPV-5 and HPV-8 resemble each other, and it led us to regard
these three viruses as one cluster and HPV-19 and HPV-25 as another.
The conclusion implies that HPV-47 as well as HPV-5 and HPV-8 is
associated with the cancer occurrence in EV. Two sets of splicing
donor and acceptor sequences in HPV-47, which were previously shown
to work in vivo, are also conserved in HPV-5 and HPV-8. One of them
allows formation of an ORF predicted to encode an E1/E4 fused
protein.
87. Favre M, Obalek S, Jablonska S, et al.:
Human papillomavirus type 49, a type isolated from flat warts of
renal transplant patients. J Virol 63(11):4909, 1989. The cloning
and characterization of the genome of human papillomavirus type 49
(HPV-49) is described. The viral DNA, which is most closely related
to the DNAs of HPVs seen in patients with epidermodysplasia
verruciformis, was aligned to the HPV-5 genome by electron
microscopic analysis of heteroduplexes between the cloned viral
DNAs.
88. Nuovo GJ, Crum CP, De Villiers EM, et al.:
Isolation of a novel human papillomavirus (type 51) from a cervical
condyloma. J Virol 62(4):1452-1455, 1988. We cloned the DNA from
a novel human papillomavirus (HPV) present in a cervical condyloma.
When DNA from this isolate was hybridized at high stringency with HPV
types 1 through 50 (HPV-1 through HPV-50), it showed weak homology
with HPV-6 and -16 and stronger homology with HPV-26. A detailed
restriction endonuclease map was prepared which showed marked
differences from the maps for other HPVs that have been isolated from
the female genital tract. Reassociation kinetic analysis revealed
that HPV-26 and this new isolate were less than 10% homologous;
hence, the new isolate is a novel strain of HPV. The approximate
positions of the open reading frames of the new strain were surmised
by hybridization with probes derived from individual open reading
frames of HPV-16. In an analysis of 175 genital biopsies from
patients with abnormal Papanicolaou smears, sequences hybridizing
under highly stringent conditions to probes from this novel HPV type
were found in 4.2, 6.1, and 2.4% of biopsies containing normal
squamous epithelium, condylomata, and intraepithelial neoplasia,
respectively. In addition, sequences homologous to probes from this
novel isolate were detected in one of five cervical carcinomas
examined.
89. Frattini MG, Lim HB, Laimins LA: In vitro
synthesis of oncogenic human papillomaviruses requires episomal
genomes for differentiation-dependent late expression. Proc Natl Acad
Sci 93(7):3062-3067, 1996. Human papillomavirus (HPV) types 16,
18, 31, and 51 are the etiologic agents of many anogenital cancers
including those of the cervix. These "high risk" HPVs specifically
target genital squamous epithelia, and their lytic life cycle is
closely linked to epithelial differentiation. We have developed a
genetic assay for HPV functions during pathogenesis using
recircularized cloned HPV 31 genomes that were transfected together
with a drug resistance marker into monolayer cultures of normal human
foreskin keratinocytes, the natural host cell. After drug selection,
cell lines were isolated that stably maintained HPV 31 DNA as
episomes and underwent terminal differentiation when grown in
organotypic raft cultures. In differentiated rafts, the expression of
late viral genes, amplification of viral DNA, and production of viral
particles were detected in suprabasal cells. This demonstrated the
ability to synthesize HPV 31 virions from transfected DNA templates
and allowed an examination of HPV functions during the vegetative
viral life cycle. We then used this system to investigate whether an
episomal genome was required for the induction of late viral gene
expression. When an HPV 31 genome (31E1*) containing a missense
mutation in the E1 open reading frame was transfected into normal
human keratinocytes, the mutant viral sequences were found to
integrate into the host cell chromosomal DNA with both early and late
regions intact. While high levels of early viral gene transcription
were observed, no late gene expression was detected in rafts of cell
lines containing the mutant viral genome despite evidence of terminal
differentiation. Therefore, the induction of late viral gene
expression required that the viral genomes be maintained as
extrachromosomal elements, and terminal differentiation alone was not
sufficient. These studies provide the basis for a detailed
examination of HPV functions during viral
pathogenesis.
90. Katase K, Teshima H, Hirai Y, et al.:
Natural history of cervical human papillomavirus lesions.
Intervirology 38(3-4):192-194, 1995. A total of 87 HPV-positive
patients with grade I and II cervical intraepithelial neoplasia (CIN
I and II) were followed up by cytology and colposcopy every 3 months
for more than 5 years following the first biopsy. These patients were
classified into three groups (progressive, persistent, and regressive
disease) according to the results. The human papillomavirus (HPV)
genome and viral types were identified by Southern blot hybridization
at Tm-40 degrees and Tm-20 degrees with DNA extracted from exfoliated
cervical cells. The lesion progressed to CIN III in 4/87 patients
(4.6%), persisted in 39 patients (44.8%), and regressed in 44
patients (50.6%). In the progressive disease group, HPV 16 was
detected in 2 patients, HPV 33 in 1 patient, and HPV 52 in 1 patient.
In the persistent disease group, HPV 58 was predominant (28%),
whereas in the regressive disease group, there was no predominant HPV
type. In 10/39 patients from the persistent disease group,
cytological examination transiently revealed severe dysplasia and/or
findings similar to carcinoma in situ. These patients showed severe
cytological abnormalities only once or twice during the follow-up.
These results suggest that the natural history of CIN possibly
depends upon the type of HPV that infects the cervix, and the
relative risk of progression was similar to that shown by previous
cross-sectional studies.
91. Rho J, Roy-Burman A, Kim H, et al.:
Nucleotide sequence and phylogenetic classification of human
papillomavirus type 59. Virology 203(1):158-161, 1994. The
complete nucleotide sequence of the HPV 59 DNA genome, isolated from
a vulvar intraepithelial neoplasia, was determined. It consists of
7896 nucleotides. A comparative analysis of this sequence with the
sequences of other HPV types revealed the closest homology to HPV 18
(71%), HPV 45 (70%), and HPV 39 (69%). Phylogenetic analysis of the
complete L1 ORFs of HPV 59 and other papillomaviruses exclusively
groups all HPVs which have been detected in mucosal lesions into one
major branch. This major branch, in turn, includes two specific
subgroups containing all high risk viruses associated with malignant
mucosal lesions. The motif in the L2 ORF
thr-thr-pro-ala-val/ile-leu/ile-asp/asn-val/ile, an extension of a
previously reported mucosal motif, is highly conserved in all HPV
types detected in mucosal lesions, whereas it is totally absent in
those viruses exclusively associated with cutaneous
lesions.
92. Egawa K, Honda Y, Inaba Y, et al.: Detection of human
papillomaviruses and eccrine ducts in palmoplantar epidermoid cysts.
Br J Dermatol 132(4):533-542, 1995. Although epidermoid cysts of
the palms and soles have long been assumed to develop following
implantation of an epidermal fragment as a result of a penetrating
injury, the pathogenic mechanism is still controversial, and the
discovery of a more common aetiological agent is awaited. Clinical,
histological, immunohistochemical and molecular biological studies
were performed on 119 epidermoid cysts of palmoplantar location, in
order to examine the role of the eccrine ducts, and human
papillomavirus (HPV), in the pathogenesis of this disorder.
Characteristic histological features were found, including
intracytoplasmic eosinophilic bodies (ICB: in 14 cases, 12%) in the
cyst wall, vacuolar structures (V: in 28 cases, 24%), or
parakeratotic nuclei (P: in 85 cases, 71%) within the keratinous mass
in the cyst cavity. Ductal structures suggesting eccrine ducts (E: in
63 cases, 53%) were also found in the cyst wall or in the cyst
cavity. Either ductal structures or carcinoembryonic antigen
expression (66 cases, 55%) were noted in a total of 73 cases (61%).
Papillomavirus common antigens were detected in 36 cases (30%)
showing one or more of the three distinct histological features, i.e.
ICB, V and P. Subsequently, hybridization experiments to detect HPV
DNA were performed in 47 cases, revealing an association between
cysts showing ICB or V and the presence of HPV 60 DNA sequences. On
the basis of our results, we propose that epidermoid cysts in the
palmoplantar regions may develop from eccrine ducts, and that HPV and
injury may play a role in their pathogenesis.
93. Kato N, Ueno H: Two cases of plantar epidermal cyst associated
with human papillomavirus. Clin Exp Dermatol 17(4):252-256, 1992.
HPV-associated epidermal cysts of the sole (HAECS) of the foot have
been reported recently in Japan in which there is positive staining
for papillomavirus antibody in the nuclei of the epithelial cells in
the cyst wall and vacuoles in the stratified horny material inside
the cysts. A causative association with a newly recognized HPV, HPV
60, has been recorded. The authors report two new cases. The possible
mechanism of cyst formation in HPV 60-infected epithelium is
discussed.
94. Matsukura T, Iwasaki T, Kawashima M: Molecular cloning of a
novel human papillomavirus (type 60) from a plantar cyst with
characteristic pathological changes. Virology 190(1):561-564,
1992. In a plantar cyst composed of the wall of the squamous cell
layer and the horny inner substance in the lower dermis, we found
characteristic pathological changes, such as cytoplasmic eosinophilic
inclusions and vacuolated structure, and, immunohistochemically, the
papillomavirus capsid antigen. The human papillomavirus (HPV) DNA
cloned from the cyst showed no homology with other known prototypes
of HPV (HPV 1 through HPV 59) by Southern blot analysis under
stringent conditions and was named as HPV 60. HPV 60 DNA was found in
three other cases of plantar cyst with the identical pathological
changes, but not in a plantar cyst without such changes. The results
suggest that HPV 60 has unique biological properties to induce a
plantar cyst as a distinct type of cutaneous HPV.
95. Honda A, Iwasaki T, Sata T, et al.: Human papillomavirus type
60-associated plantar wart. Ridged wart. Arch Dermatol
130(11):1413-1417, 1994. BACKGROUND: We had recently cloned a new
cutaneous human papillomavirus type 60 (HPV-60) from a plantar cyst
with characteristic pathologic changes and identified it in
additional cysts. However, it is not known whether or not HPV-60
infection causes the other cutaneous lesions. OBSERVATIONS: Six
plantar warts were found in five patients. These warts were found
either with concomitant plantar cysts (four patients) or without an
accompanying cyst (one patient). All warts showed a similar clinical
appearance, including a smooth and slightly elevated surface and the
retained appearance of the dermal ridges. Their histopathologic
features were identical to those found in the wall of the cysts
reported previously, namely hyperkeratosis with vacuolated structure
with or without nuclei in the horny layer and amorphous eosinophilic
cytoplasmic inclusions in the cells with peripherally located nuclei
in the granular and prickle cell layers. By Southern blot analysis,
all warts were found to harbor HPV-60 DNA. In addition,
immunohistochemistry and in situ hybridization analysis revealed the
presence of viral capsid antigen and viral genome in these lesions,
respectively. CONCLUSION: We conclude that HPV-60 infection on the
plantar skin causes the warty lesion, designated as ridged wart,
distinct from those infected with other cutaneous human
papillomaviruses.
96. Egawa K: New types of human papillomaviruses
and intracytoplasmic inclusion bodies: a classification of inclusion
warts according to clinical features, histology and associated HPV
types. Br J Dermatol 130(2):158-166, 1994. Two new types of
intracytoplasmic inclusion bodies (ICBs) associated with distinct
clinical features, and the presence of DNA of distinct types of human
papillomaviruses (HPVs) are reported. One hundred and seven cutaneous
warts containing ICBs were grouped into three categories according to
distinct clinicopathological features: 67 were wart lesions with
well-known granular (Gr)-ICB, 13 were punctate keratotic lesions with
filamentous (Fl)-ICB and 31 were pigmented warts with homogeneous
(Hg)-ICB. Molecular biological studies were performed in order to
assess a specific association of each group of warts with distinct
types of HPV. HPV-1 DNA sequences were detected in all the lesions
with a Gr-ICB. Punctate keratotic lesions with Fl-ICB were associated
with HPV-63, which was newly cloned from such a lesion. One of the
samples also contained HPV-1 DNA. Pigmented warts with Hg-ICBs
contained one of the related HPVs, i.e. HPV-4, HPV-60 or a novel type
of HPV, HPV-65. Based on these associations, a classification of
inclusion warts is proposed.
97. Egawa K, Delius H, Matsukura T, et al.: Two
novel types of human papillomavirus, HPV 63 and HPV 65: comparisons
of their clinical and histological features and DNA sequences to
other HPV types. Virology 194(2):789-799, 1993. An
association exists between verrucae presenting with specific
histological features and the type of HPV inducing the lesion. An HPV
1 induced lesion is associated with a granular type of
intracytoplasmic inclusion body (Gr-ICB), whereas HPV 4 is associated
with the homogeneous type of ICB (Hg-ICB). A third type of inclusion
body, a filamentous type (F1-ICB), was found to be present in
multiple punctate keratotic lesions. A novel type of papillomavirus,
HPV 63, was present in such lesions. After cloning, characterization
and sequencing of its DNA genome, HPV 63, although still very
distinct (< 66% nucleotide homology), could be grouped with HPV 1.
Upon histological examination of verrucous lesions presenting
clinically with grey to black pigmentation, the Hg-ICB present were
very characteristic. These lesions were infected with HPV 4, HPV 60,
or HPV 65. The majority of the lesions contained the novel type HPV
65. This viral DNA was isolated and characterized. Its DNA sequence
has an 83% homology to that of HPV 4, whereas both are more distantly
related to HPV 60, an HPV isolated from an epidermoid
cyst.
98. Forslund O, Hansson BG: Human papillomavirus
type 70 genome cloned from overlapping PCR products: complete
nucleotide sequence and genomic organization. J Clin Microbiol
34(4):802-809, 1996. The genome of human papillomavirus (HPV)
type 70 (HPV 70), isolated from a cervical condyloma, was obtained by
cloning overlapping PCR products. By automated DNA sequence analysis,
the genome was found to consist of 7,905 bp with a G + C content of
40%. The genomic organization showed the characteristic features
shared by other sequenced HPVs. Nucleotide sequence comparison with
previously known HPV types demonstrated the closest homology with HPV
68 (82%), HPV 39 (82%), HPV 18 (70%), HPV 45 (70%), and HPV 59 (70%).
Comparison with seven other partially sequenced HPV 70 isolates
showed homologies of between 100 and 99.5%. Cloning of overlapping
PCR products and automated DNA sequence analysis was found to be a
feasible method of obtaining full-length sequences of
HPVs.
99. Volter C, He Y, Delius H, et al.: Novel HPV
types present in oral papillomatous lesions from patients with HIV
infection. Int J Cancer 66(4):453-456, 1996. Patients infected
with the human immunodeficiency virus (HIV) often develop multiple
papillomatous lesions of the oral cavity. In the present study, a
total of 67 biopsies from benign oral lesions were analyzed for the
presence of human papillomavirus (HPV) DNA using Southern-blot
hybridization in combination with a polymerase chain reaction
designed to detect all known HPV types, as well as unidentified
types. These samples, collected at random from a high-risk
population, were subsequently divided into 57 biopsies originating
from patients with confirmed HIV infection and 10 biopsies from
patients with unknown HIV status. Each sample was amplified with 7
different combinations of degenerate primers. All amplified products
were sequenced. HPV DNA sequences were detected in 67% (45/67) of the
samples. HPV 7 (19%) and HPV 32 (28%) were the predominant HPV types.
HPV 32 was present in 2/4 fibromas tested. Two new HPV types, HPV 72
and HPV 73, were identified in oral warts with atypia. The complete
genomes of these viruses were cloned and sequenced. Other HPV types
detected were HPV 2a, HPV 6b, HPV 13, HPV 16, HPV 18, HPV 55, HPV 59
and HPV 69.
100. West AB, Soloway GN, Lizarraga G, et al.:
Type 73 human papillomavirus in esophageal squamous cell carcinoma: a
novel association. Cancer 77(12):2440-2444, 1996. BACKGROUND:
Human papillomaviruses (HPVs) commonly cause proliferative lesions of
squamous epithelia, and infection with certain HPV types carries a
high risk of malignant transformation, especially in the uterine
cervix but also at other sites, including the esophagus. We used
molecular techniques to detect and type HPV in an in situ squamous
cell carcinoma in the esophagus of a 39-year old woman. METHODS: DNA
was extracted from paraffin sections of the esophageal lesion and of
the uterine cervix (which was removed several years earlier), and
analyzed for HPV by polymerase chain reaction (PCR). Primers
complementary to highly conserved regions of the open reading frame
of most genital HPVs were used to amplify a approximately 450 base
pair product that contained both conserved and divergent regions. The
PCR products were hybridized with probes specific for HPV-6, HPV-11,
HPV-16, and HPV-18, and with a consensus probe. A conspicuous band in
the esophageal sample failed to hybridize with any of the probes. The
amplimer was subcloned and sequenced. The sequence was compared with
other known HPVs. RESULTS: The intraepithelial neoplasia in the
patient's cervical cone biopsy contained HPV-16. The esophageal
lesion contained HPV that did not hybridize with probes for types 6,
11, 16, or 18, but exhibited 98.3% homology with HPV-73. CONCLUSIONS:
Squamous cell carcinoma in situ of the esophagus may be associated
with infection by HPV-73.
© 1995-2000 The Internet Dermatology Society, Inc. All rights
reserved.
Send your comments to: textbook@telemedicine.org
{kind=link}
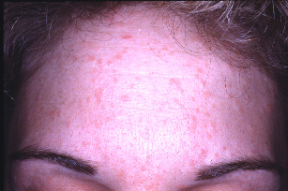{kind=link}
{kind=link}