
![]()
|
|
| ||
Other relevant laboratory tests: ANF positive (speckled)
1:640. Anti-DNA (double stranded) 1:512 mid positive. SSB/La 6.065
high positive.
|
Extended Clinical Course: |
Click on the image for magnification |
|
A further relapse followed at the beginning of May. Targetoid and annular erythematous purpuric lesions were seen on the upper chest, arms, forearms, hands, thighs and legs. | |
|
Perniotic lesions with ulceration were seen on her fingertips. |
Laboratory Examinations: ANF positive (speckled) 1:160.
Anti-DNA (double stranded) 2.133 high positive. SSB/La 6.335 mid
positive.
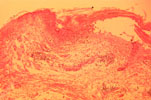
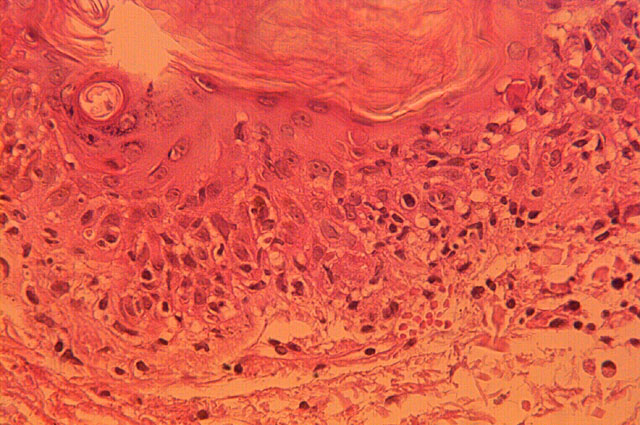
Histology, June 1996: At a further relapse at the beginning of
June skin biopsies were taken from the right arm, from lesional and
normal skin for histopathology and immunofluorescence. Histology (Dr.
J.A. Posen): There is focal surface parakeratosis. The epidermis in
areas shows some degree of basal degeneration and the upper dermis is
edematous with an increase in vascularity and a patchy mild
lymphohistiocytic infiltrate. Some pigmentary incontinence is
present. No epidermal necrosis or isolated necrotic cells are
identified. The histologic features are in keeping with a diagnosis
of lupus erythematosus.


Immunofluorescence: (Dr. W. Grayson, The South African
Institute for Medical Research). Direct and Indirect
immunofluorescence of lesional and normal skin was essentially
non-specific.
Response to treatment: The patient has been treated with
different combinations of oral and topical corticosteroids and oral
and topical antibiotics. she has improved whenever on treatement but
has had several relapses. However the intervals between relapses are
becoming longer.
![]() EMAIL your diagnosis to
the Internet Dermatology
Society.
EMAIL your diagnosis to
the Internet Dermatology
Society.
![]() If you mail in your case, please include the appropriate
clinical and pathology slides to be scanned in.
If you mail in your case, please include the appropriate
clinical and pathology slides to be scanned in.
Global Dermatology Grand Rounds
Rhett J. Drugge, M.D., Founding Editor
50 Glenbrook Road
Stamford, CT 06902 USA
Phone: (203) 324-5719
![]() If you email your case, please include compressed jpeg
or gif images to:
rdrugge[AT_SIGN_HERE]telemedicine.org.
If you email your case, please include compressed jpeg
or gif images to:
rdrugge[AT_SIGN_HERE]telemedicine.org.
Thanks
for your participation!






